

The impact of mouth breathing on dentofacial development: A concise review
- PMID: 36159237
- PMCID: PMC9498581
- DOI: 10.3389/fpubh.2022.929165
The impact of mouth breathing on dentofacial development: A concise review
Abstract
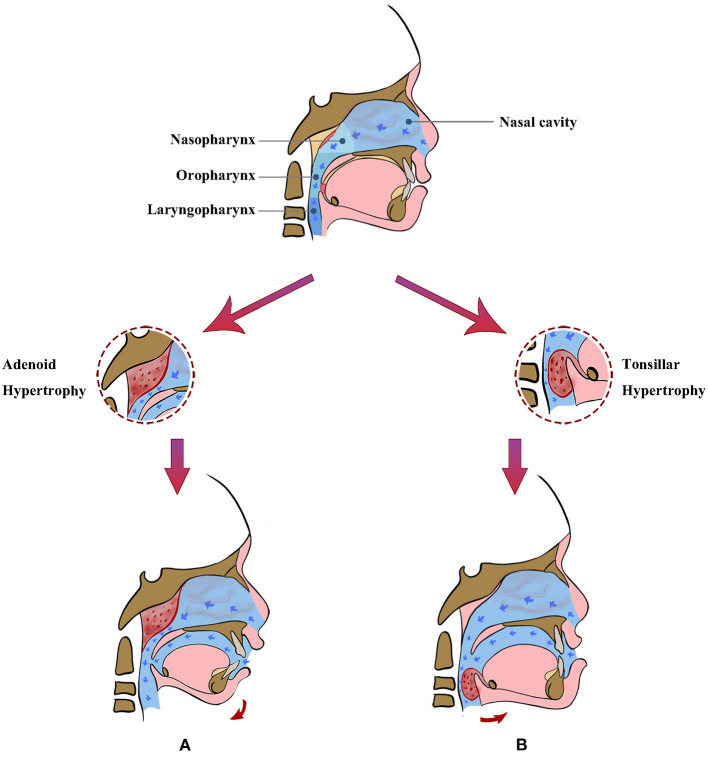
Mouth breathing is one of the most common deleterious oral habits in children. It often results from upper airway obstruction, making the air enter completely or partially through oral cavity. In addition to nasal obstruction caused by various kinds of nasal diseases, the pathological hypertrophy of adenoids and/or tonsils is often the main etiologic factor of mouth breathing in children. Uncorrected mouth breathing can result in abnormal dental and maxillofacial development and affect the health of dentofacial system. Mouth breathers may present various types of growth patterns and malocclusion, depending on the exact etiology of mouth breathing. Furthermore, breathing through the oral cavity can negatively affect oral health, increasing the risk of caries and periodontal diseases. This review aims to provide a summary of recent publications with regard to the impact of mouth breathing on dentofacial development, describe their consistencies and differences, and briefly discuss potential reasons behind inconsistent findings.
Keywords: adenoids; malocclusion; maxillofacial development; mouth breathing; palatine tonsil.
Copyright © 2022 Lin, Zhao, Qin, Hua and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effect of diseases of tonsils and adenoids on dentofacial morphology.Ann Otol Rhinol Laryngol. 1975 Mar-Apr;84(2 PT2 SUPPL 19):50-4. doi: 10.1177/00034894750840S212. Ann Otol Rhinol Laryngol. 1975. PMID: 1130772 No abstract available.
-
Variation of patterns of malocclusion by site of pharyngeal obstruction in children.Arch Otolaryngol Head Neck Surg. 2010 Nov;136(11):1116-20. doi: 10.1001/archoto.2010.187. Arch Otolaryngol Head Neck Surg. 2010. PMID: 21079167
-
Adenotonsillar hypertrophy as a risk factor of dentofacial abnormality in Korean children.Eur Arch Otorhinolaryngol. 2015 Nov;272(11):3311-6. doi: 10.1007/s00405-014-3407-6. Epub 2014 Dec 10. Eur Arch Otorhinolaryngol. 2015. PMID: 25490975
-
The effects of adenoid hypertrophy and oral breathing on maxillofacial development: a review of the literature.J Clin Pediatr Dent. 2024 Jan;48(1):1-6. doi: 10.22514/jocpd.2024.001. Epub 2024 Jan 3. J Clin Pediatr Dent. 2024. PMID: 38239150 Review.
-
Impact of adenotonsillectomy on the dentofacial development of obstructed children: a systematic review and meta-analysis.Eur J Orthod. 2017 Oct 1;39(5):509-518. doi: 10.1093/ejo/cjx005. Eur J Orthod. 2017. PMID: 28379334
Cited by
-
[The current status and expectation of pediatric total facial management].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023 Aug;37(8):619-621. doi: 10.13201/j.issn.2096-7993.2023.08.003. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023. PMID: 37551567 Free PMC article. Chinese.
-
[Pediatric oral maxillofacial management and artificial intelligence].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023 Aug;37(8):658-661. doi: 10.13201/j.issn.2096-7993.2023.08.012. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023. PMID: 37551576 Free PMC article. Review. Chinese.
-
Functional therapy and adenotonsillectomy clinical trial for class II malocclusion (FACT-II): protocol for a randomised controlled trial.BMJ Open. 2024 Apr 16;14(4):e079571. doi: 10.1136/bmjopen-2023-079571. BMJ Open. 2024. PMID: 38626960 Free PMC article.
-
The Therapeutic Approaches Dealing with Malocclusion Type III-Narrative Review.Life (Basel). 2025 May 22;15(6):840. doi: 10.3390/life15060840. Life (Basel). 2025. PMID: 40566493 Free PMC article. Review.
-
CBCT study of adenoid and nasopharyngeal airway in boys with unilateral complete cleft lip and palate.Oral Radiol. 2025 Aug 30. doi: 10.1007/s11282-025-00851-0. Online ahead of print. Oral Radiol. 2025. PMID: 40885817
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical