

ST-segment elevation myocardial infarction in Kawasaki disease: A case report and review of literature
- PMID: 36159436
- PMCID: PMC9477670
- DOI: 10.12998/wjcc.v10.i26.9368
ST-segment elevation myocardial infarction in Kawasaki disease: A case report and review of literature
Abstract
Background: Kawasaki disease (KD) is an acute self-limiting febrile vasculitis that occurs during childhood and can cause coronary artery aneurysm (CAA). CAAs are associated with a high rate of adverse cardiovascular events.
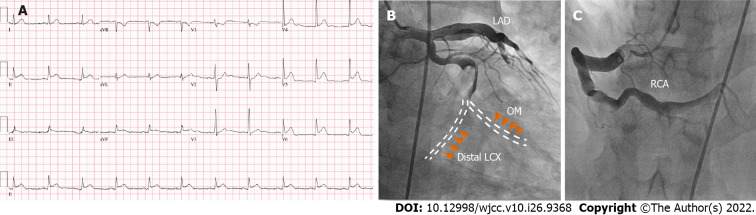
Case summary: A Korean 35-year-old man with a 30-year history of KD presented to the emergency room with chest pain. Emergent coronary angiography was performed as ST-segment elevation in the inferior leads was observed on the electrocardiogram. An aneurysm of the left circumflex (LCX) coronary artery was found with massive thrombi within. A drug-eluting 4.5 mm 23 mm-sized stent was inserted into the occluded area without complications. The maximal diameter of the LCX was 6.0 mm with a Z score of 4.7, suggestive of a small aneurysm considering his age, sex, and body surface area. We further present a case series of 19 patients with KD, including the current patient, presenting with acute coronary syndrome (ACS). Notably, none of the cases showed Z scores; only five patients (26%) had been regularly followed up by a physician, and only one patient (5.3%) was being treated with antithrombotic therapy before ACS occurred.
Conclusion: For KD presenting with ACS, regular follow up and medical therapy may be crucial for improved outcomes.
Keywords: Acute coronary syndrome; Case report; Coronary angiography; Kawasaki disease; Percutaneous coronary intervention; ST elevation myocardial infarction.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have nothing to disclose.
Figures


Similar articles
-
Medium-Term Complications Associated With Coronary Artery Aneurysms After Kawasaki Disease: A Study From the International Kawasaki Disease Registry.J Am Heart Assoc. 2020 Aug 4;9(15):e016440. doi: 10.1161/JAHA.119.016440. Epub 2020 Jul 28. J Am Heart Assoc. 2020. PMID: 32750313 Free PMC article.
-
A Young Patient With Acute Ostial Right Coronary Artery Aneurysm Presenting As ST Elevation Myocardial Infarction.Cureus. 2024 Apr 11;16(4):e58063. doi: 10.7759/cureus.58063. eCollection 2024 Apr. Cureus. 2024. PMID: 38741823 Free PMC article.
-
Acute Adult-Onset Kawasaki Disease Complicated by Coronary Artery Aneurysms, Thrombosis, and ST-Segment Elevation Myocardial Infarction.JACC Case Rep. 2021 Feb 10;3(2):276-279. doi: 10.1016/j.jaccas.2020.11.034. eCollection 2021 Feb. JACC Case Rep. 2021. PMID: 34317517 Free PMC article.
-
API expert consensus document on management of ischemic heart disease.J Assoc Physicians India. 2006 Jun;54:469-80. J Assoc Physicians India. 2006. PMID: 16909697 Review.
-
Contemporary NSTEMI management: the role of the hospitalist.Hosp Pract (1995). 2020 Feb;48(1):1-11. doi: 10.1080/21548331.2020.1701329. Epub 2020 Feb 20. Hosp Pract (1995). 2020. PMID: 31815570 Review.
Cited by
-
When two Z-scores meet-analysis of exercise capacity of children and adolescents with Kawasaki disease by a new Z-score model of coronary artery and a new Z-score evaluating peak oxygen consumption : Coronary artery Z-score and peakVO2 Z-score in KD.Ital J Pediatr. 2023 Sep 29;49(1):129. doi: 10.1186/s13052-023-01535-3. Ital J Pediatr. 2023. PMID: 37773131 Free PMC article.
-
Imperative for long-term management and surveillance in Kawasaki disease.World J Clin Cases. 2025 Feb 6;13(4):99637. doi: 10.12998/wjcc.v13.i4.99637. World J Clin Cases. 2025. PMID: 39917574 Free PMC article.
References
-
- Burns JC, Glodé MP. Kawasaki syndrome. Lancet. 2004;364:533–544. - PubMed
-
- Nakamura Y. Kawasaki disease: epidemiology and the lessons from it. Int J Rheum Dis. 2018;21:16–19. - PubMed
-
- Kim GB, Park S, Eun LY, Han JW, Lee SY, Yoon KL, Yu JJ, Choi JW, Lee KY. Epidemiology and Clinical Features of Kawasaki Disease in South Korea, 2012-2014. Pediatr Infect Dis J. 2017;36:482–485. - PubMed
-
- Wu MH, Chen HC, Yeh SJ, Lin MT, Huang SC, Huang SK. Prevalence and the long-term coronary risks of patients with Kawasaki disease in a general population <40 years: a national database study. Circ Cardiovasc Qual Outcomes. 2012;5:566–570. - PubMed
-
- Abrams JY, Belay ED, Uehara R, Maddox RA, Schonberger LB, Nakamura Y. Cardiac Complications, Earlier Treatment, and Initial Disease Severity in Kawasaki Disease. J Pediatr. 2017;188:64–69. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
