

Adaptive immunity in different CT patterns of active tuberculosis and possible variability according to patients' geographic provenience
- PMID: 36160177
- PMCID: PMC9489992
- DOI: 10.3389/fmed.2022.890609
Adaptive immunity in different CT patterns of active tuberculosis and possible variability according to patients' geographic provenience
Abstract
Background: It is still unclear if low lymphocyte levels are directly related to immunological modifications induced by the TB infection or if they depend on the general pre-existing health impairment of affected patients. Our aim was to detect eventual differences in the immunological status of patients with pulmonary TB compared to an age and sex-matched group of hospitalized patients with other bacterial community-acquired pneumonia (CAP). In addition, we tried to assess an association between alterations in the peripheral lymphocyte subsets and the development of different CT patterns of active TB and to discover differences in the immunological status and in the radiological patterns of TB presentation between patients of different geographic proveniences.
Methods: This observational study included 48 patients with TB and 48 sex- and age-matched patients affected by other bacterial CAP. The presence of HIV/AIDS, other immunocompromising conditions, and confounding chronic pulmonary comorbidities was excluded. Flow cytometry was performed on all the enrolled subjects at admission, before starting the appropriate antibiotic therapy. Patients with TB also underwent a computed tomography (CT) scan.
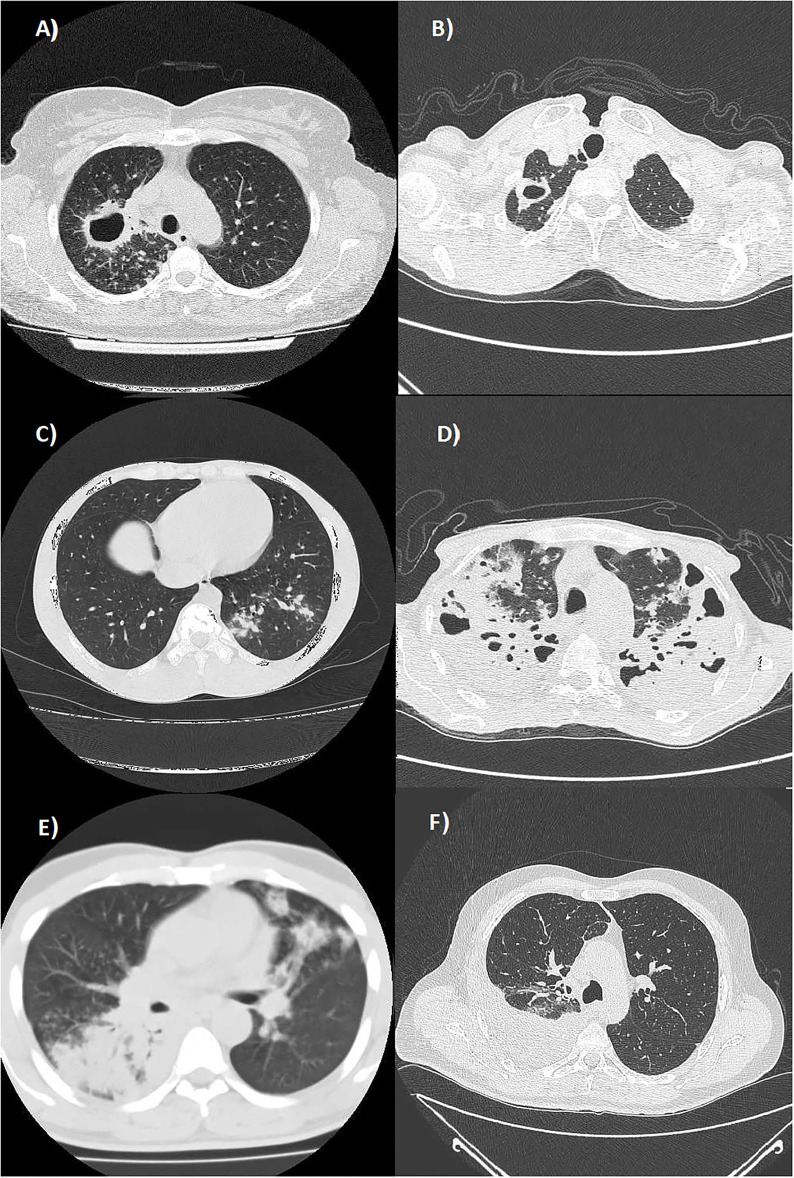
Results: Patients with TB showed a decrease in the absolute count of all the lymphocyte subsets compared to the CAP group. Only the reduction in the percentage of CD4+ T-lymphocytes was significant, while the percentage of CD8+ T-lymphocytes was significantly increased. Patients presenting exudative forms with atypical locations of TB showed a significant reduction in the absolute count and percentage of CD19+ B-lymphocytes compared to those affected by productive TB forms with the typical location. Despite being younger, our black Sub-Saharan Africans showed a significant reduction in the CD4+ T-lymphocytes compartment and a higher prevalence of atypical and exudative forms of TB compared with white Europeans.
Conclusion: Tuberculosis itself may alter peripheral blood lymphocyte subsets compared to other CAP. An impaired CD19+ B-lymphocyte compartment may result in an abnormal exudative response in atypical locations and a suboptimal bacterial control. Other constitutive or environmental causes may influence immunological differences found in patients with TB, particularly in case of different geographic origins. Anyhow, flow cytometry may be of great value in evaluating the immune function of these patients.
Keywords: CT pattern; adaptive immunity; flow cytometry; geographic provenience; tuberculosis.
Copyright © 2022 Scioscia, Lacedonia, Giuffreda, Caccavo, Quarato, Soccio, Tondo, Sassani, Pescatore and Foschino Barbaro.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- World Health Organization . Global Tuberculosis Report. (2021). Available online at: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/globa... (accessed February 24, 2022).
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous