

Therapeutic strategies for post-transplant recurrence of hepatocellular carcinoma
- PMID: 36160651
- PMCID: PMC9494935
- DOI: 10.3748/wjg.v28.i34.4929
Therapeutic strategies for post-transplant recurrence of hepatocellular carcinoma
Abstract
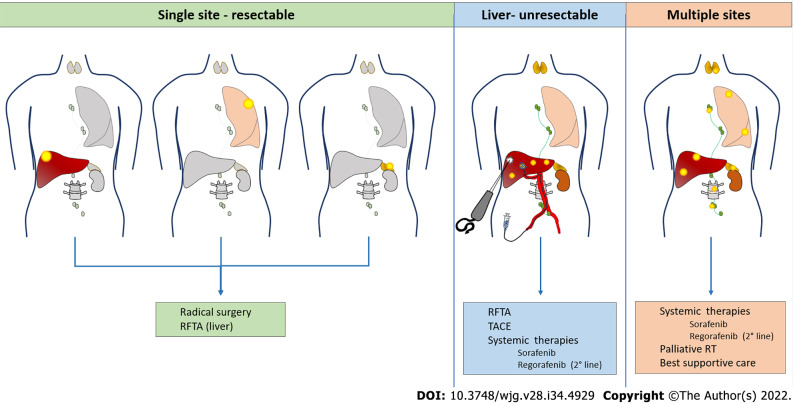
Despite stringent selection criteria, hepatocellular carcinoma recurrence after liver transplantation (LT) still occurs in up to 20% of cases, mostly within the first 2-3 years. No adjuvant treatments to prevent such an occurrence have been developed so far. However, a balanced use of immunosuppression with minimal dose of calcineurin inhibitors and possible addition of mammalian target of rapamycin inhibitors is strongly advisable. Moreover, several pre- and post-transplant predictors of recurrence have been identified and may help determine the frequency and duration of post-transplant follow-up. When recurrence occurs, the outcomes are poor with a median survival of 12 mo according to most retrospective studies. The factor that most impacts survival after recurrence is timing (within 1-2 years from LT according to different authors). Several therapeutic options may be chosen in case of recurrence, according to timing and disease presentation. Surgical treatment seems to provide a survival benefit, especially in case of late recurrence, while the benefit of locoregional treatments has been suggested only in small retrospective studies. When systemic treatment is indicated, sorafenib has been proved safe and effective, while only few data are available for lenvatinib and regorafenib in second line. The use of immune checkpoint inhibitors is controversial in this setting, given the safety warnings for the risk of acute rejection.
Keywords: Hepatocellular carcinoma; Immunosuppression; Liver transplantation; Locoregional treatment; Recurrence; Surgical treatment; Systemic treatment.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
References
-
- Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019;380:1450–1462. - PubMed
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
