

Surgical Management of Postoperative Grade C Pancreatic Fistula following Pancreatoduodenectomy
- PMID: 36160826
- PMCID: PMC9421704
- DOI: 10.1159/000521727
Surgical Management of Postoperative Grade C Pancreatic Fistula following Pancreatoduodenectomy
Abstract
Background: The incidence of Grade C postoperative pancreatic fistula ranges from 2 to 11% depending on the type of pancreatic resection. This complication may frequently require early relaparotomy and the surgical approach remains technically challenging and is still associated with a high mortality. Infectious complications and post-operative hemorrhage are the two most common causes of reoperation.
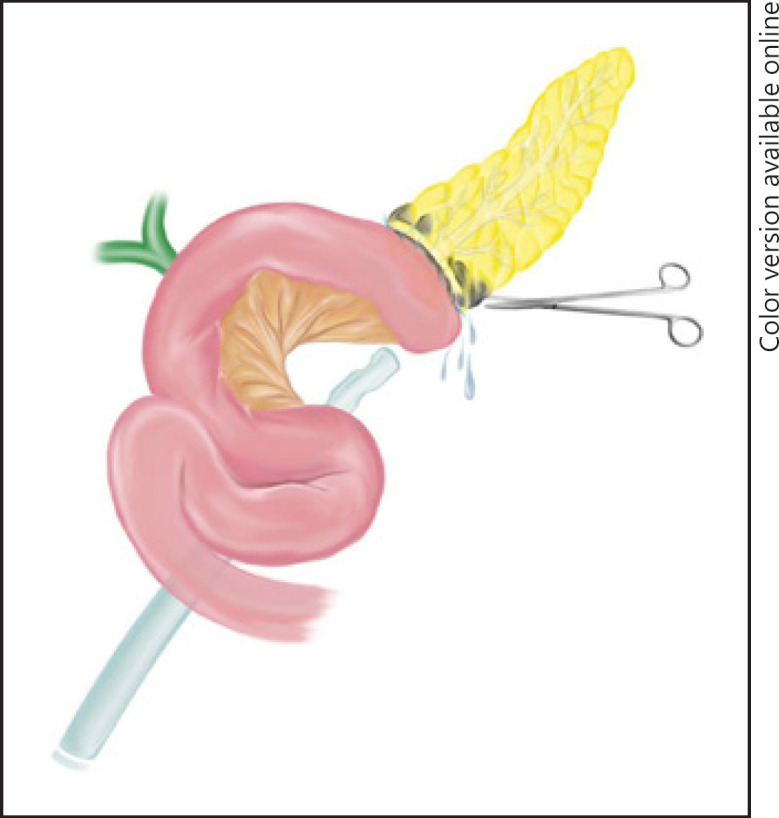
Summary: The best management of grade C pancreatic fistulas remains controversial and ranges from conservative approaches up to completion pancreatectomy. The choice of the technique depends on the patient's conditions, intraoperative findings, and surgeon's discretion. A pancreas-preserving strategy appears to be attractive, including from simple to more complex procedures such as debridement and drainage, and external wirsungostomy. Completion pancreatectomy should be reserved for selected cases, including stable patients with severe infection complication or hemorrhage after pancreatic fistula who do not respond to pancreas-preserving procedures.
Key messages: This review describes the current options for management of grade C pancreatic fistula after pancreatoduodenectomy with regard to indication, choice of procedure and outcomes of the different approaches.
Keywords: Grade C fistula; Pancreatic fistula; Pancreatoduodenectomy; Postoperative pancreatic fistula; Surgical management; Whipple.
Copyright © 2022 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures





References
-
- Fuks D, Piessen G, Huet E, Tavernier M, Zerbib P, Michot F, et al. Life-threatening postoperative pancreatic fistula (grade C) after pancreaticoduodenectomy: incidence, prognosis, and risk factors. Am J Surg. 2009;197((6)):702–9. - PubMed
-
- Miyagawa S, Makuuchi M, Kawasaki S, Ogiwara M. Second-stage pancreatojejunostomy following pancreatoduodenectomy in high-risk patients. Am J Surg. 1994;168:66–8. - PubMed
-
- Zhou YM, Zhou X, Wan T, Xu D, Si XY. An evidence-based approach to the surgical interventions for severe pancreatic fistula after pancreatoduodenectomy. Surgeon. 2018;16((2)):119–24. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
