

A method for detailed determination of hospital surge capacity: a prerequisite for optimal preparedness for mass-casualty incidents
- PMID: 36163513
- PMCID: PMC9512961
- DOI: 10.1007/s00068-022-02081-z
A method for detailed determination of hospital surge capacity: a prerequisite for optimal preparedness for mass-casualty incidents
Erratum in
-
Correction: A method for detailed determination of hospital surge capacity: a prerequisite for optimal preparedness for mass-casualty incidents.Eur J Trauma Emerg Surg. 2023 Apr;49(2):633-634. doi: 10.1007/s00068-022-02133-4. Eur J Trauma Emerg Surg. 2023. PMID: 36598542 Free PMC article. No abstract available.
Abstract
Background: Defined goals for hospitals' ability to handle mass-casualty incidents (MCI) are a prerequisite for optimal planning as well as training, and also as base for quality assurance and improvement. This requires methods to test individual hospitals in sufficient detail to numerically determine surge capacity for different components of the hospitals. Few such methods have so far been available. The aim of the present study was with the use of a simulation model well proven and validated for training to determine capacity-limiting factors in a number of hospitals, identify how these factors were related to each other and also possible measures for improvement of capacity.
Materials and methods: As simulation tool was used the MACSIM® system, since many years used for training in the international MRMI courses and also successfully used in a pilot study of surge capacity in a major hospital. This study included 6 tests in three different hospitals, in some before and after re-organisation, and in some both during office- and non-office hours.
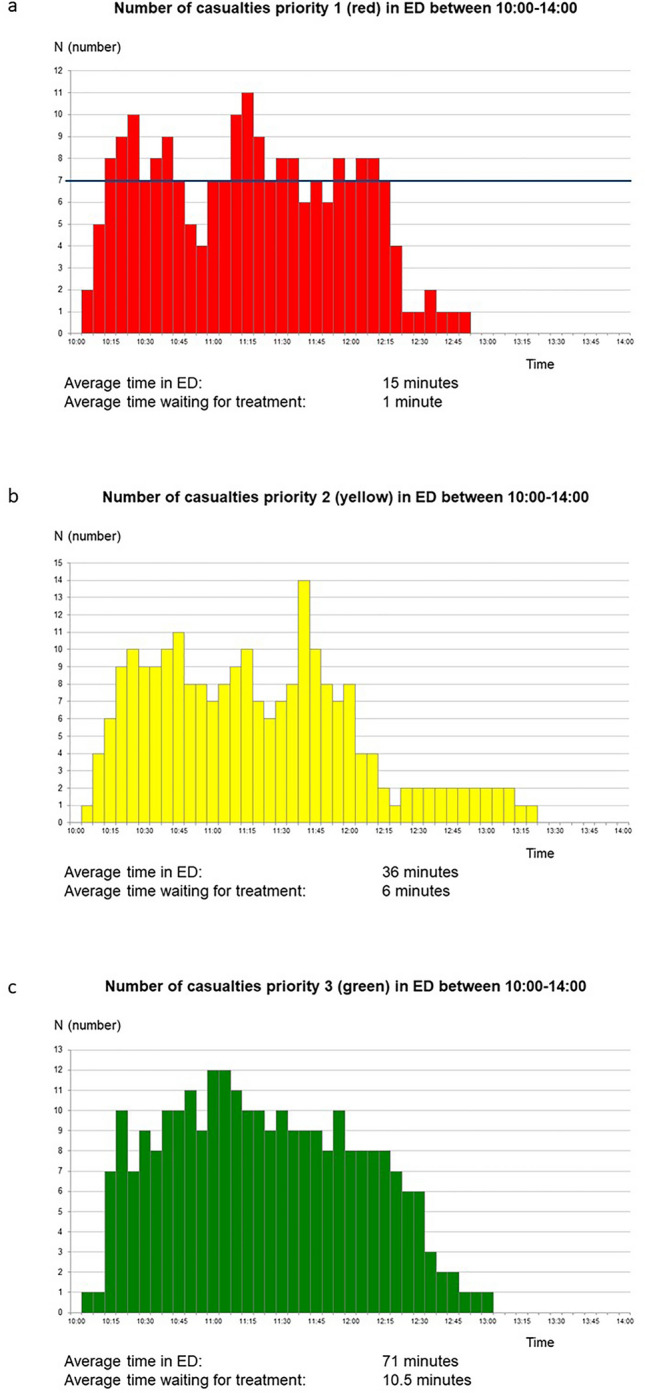
Results: The primary capacity-limiting factor in all hospitals was the capacity to handle severely injured patients (major trauma) in the emergency department. The load of such patients followed in all the tests a characteristic pattern with "peaks" corresponding to ambulances return after re-loading. Already the first peak exceeded the hospitals capacity for major trauma, and the following peaks caused waiting times for such patients leading to preventable mortality according to the patient-data provided by the system. This emphasises the need of an immediate and efficient coordination of the distribution of casualties between hospitals. The load on surgery came in all tests later, permitting either clearing of occupied theatres (office hours) or mobilising staff (non-office hours) sufficient for all casualties requiring immediate surgery. The final capacity-limiting factors in all tests was the access to intensive care, which also limited the capacity for surgery. On a scale 1-10, participating staff evaluated the accuracy of the methodology for test of surge capacity to MD 8 (IQR 2), for improvement of disaster plans to MD 9 (IQR 2) and for simultaneous training to MD 9 (IQR 3).
Conclusions: With a simulation system including patient data with a sufficient degree of detail, it was possible to identify and also numerically determine the critical capacity-limiting factors in the different phases of the hospital response to MCI, to serve as a base for planning, training, quality control and also necessary improvement to rise surge capacity of the individual hospital.
Keywords: Disaster; Hospital capacity; Hospital contingency; Hospital preparedness; Major incident; Mass casualty incident; Simulation; Surge capacity; Training.
© 2022. The Author(s).
Conflict of interest statement
One of the authors (KLM) has copyright to the MACSIM® simulation system used in this study.
Figures








References
-
- Lennquist S. Major incidents—definitions and demands on the health care system. In: Lennquist (ed) Medical response to major incidents and disasters. Springer (Berlin/London/New York) 2012; 1:1–8
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
