

Comparative Evaluation of Efficacy and Safety of the Diode Laser (980 nm) and Sclerotherapy for the Treatment of Oral Pyogenic Granuloma
- PMID: 36164597
- PMCID: PMC9509284
- DOI: 10.1155/2022/8269221
Comparative Evaluation of Efficacy and Safety of the Diode Laser (980 nm) and Sclerotherapy for the Treatment of Oral Pyogenic Granuloma
Abstract
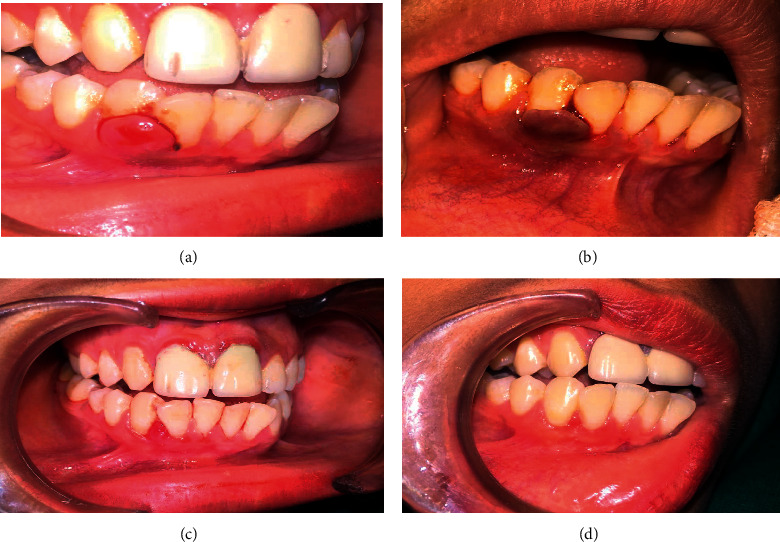
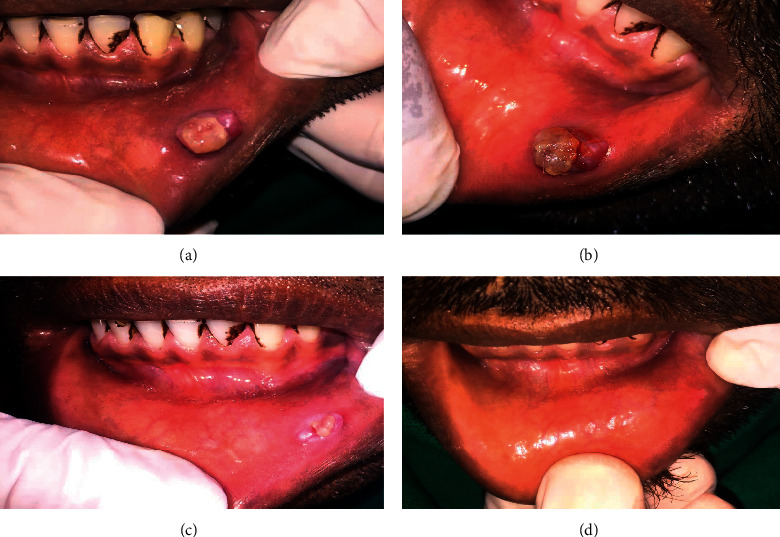
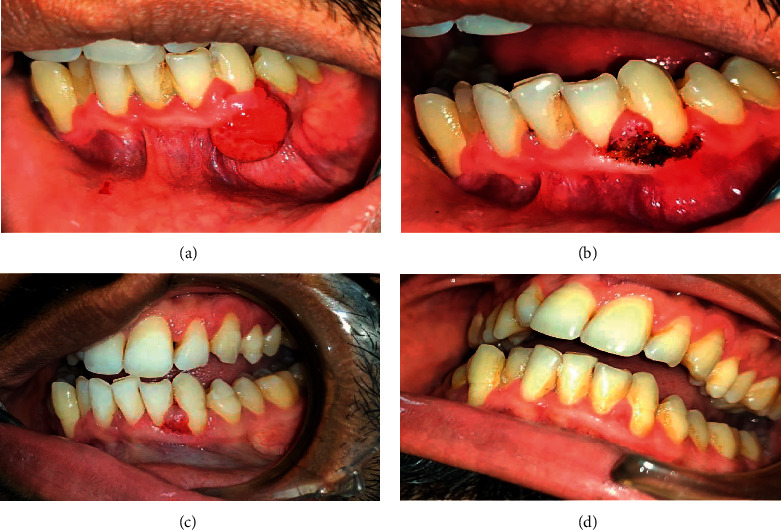
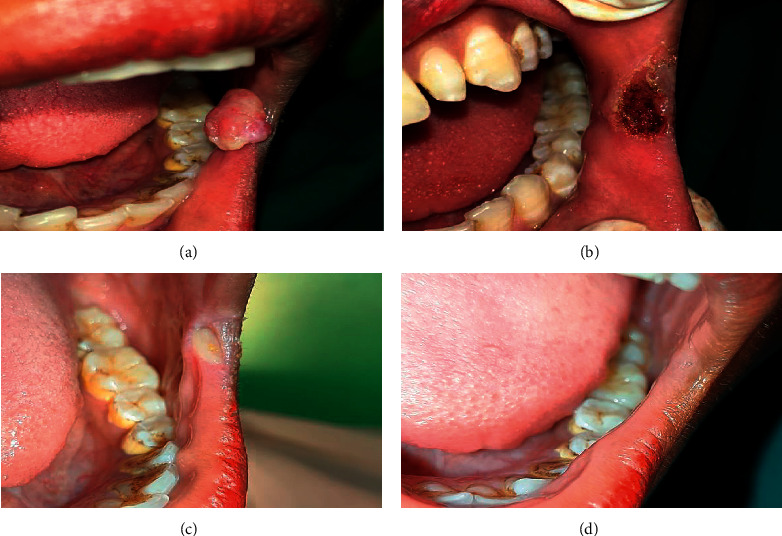
Background: Pyogenic granuloma (PG) is a tumor-like, non-neoplastic lesion of the soft tissue that commonly appears in the oral cavity. Various treatment modalities have been discussed, including surgical excision, cryosurgery, curettage, electrodessication, corticosteroid injection, sclerotherapy, and lasers. This observational retrospective study compared effectiveness between diode lasers and sclerotherapy for PG treatment.
Materials and methods: From July 2016 to January 2021, data of oral PG cases treated with sclerotherapy and diode lasers were gathered. Patients were evaluated and categorized according to their gender, sex, site of lesions, size of lesions, number of sessions, details of side effects, details of the VAS (Visual Analogue Scale) on third postoperative day, response of treatment to individual groups, time required for complete resolution, and details of recurrence. Inferential statistical analysis was performed.
Results: We included 73 patients, of whom 43 and 30 received laser and sclerotherapy treatment, respectively. Compared with the sclerotherapy group, the laser group had less side effects including pain, edema, ulceration, ecchymosis, infections, and scarring. The difference in postoperative pain (VAS scale) between the groups was statistically significant (p-value 0.004). Complete remission was seen in the laser group, while 3 cases of the sclerotherapy group had no response (p-value -0.034). The laser group experienced greater recurrence than did the sclerotherapy group.
Conclusions: Both sclerotherapy with laser and 3% sodium tetradecyl sulfate are effective for treating oral PG. Sclerotherapy is more effective in preventing recurrence. In terms of side effects, diode lasers are superior to sclerotherapy.
Copyright © 2022 Peeyush Shivhare et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Gordón-Núñez M. A., Vasconcelos Carvalho M., Benevenuto T. G., Lopes M. F. F., Silva L. M. M., Galvão H. C. Oral pyogenic granuloma: a retrospective analysis of 293 cases in a Brazilian population. Journal of Oral and Maxillofacial Surgery . 2010;68(9):2185–2188. doi: 10.1016/j.joms.2009.07.070. - DOI - PubMed
-
- Shivhare P., Parihar A. Textbook of Oral Medicine and Radiology . Hyderabad, India: Paras publisher; 2021. Benign and malignant non-odontogenic tumors of oral cavity.
-
- Shivhare P., Singh V., Singh A. Use of sodium tetradecyl sulphate for treatment of oral lesions. Journal of College of Medical Sciences—Nepal . 2019;15(4):282–286. doi: 10.3126/jcmsn.v15i4.26206. - DOI
LinkOut - more resources
Full Text Sources
