

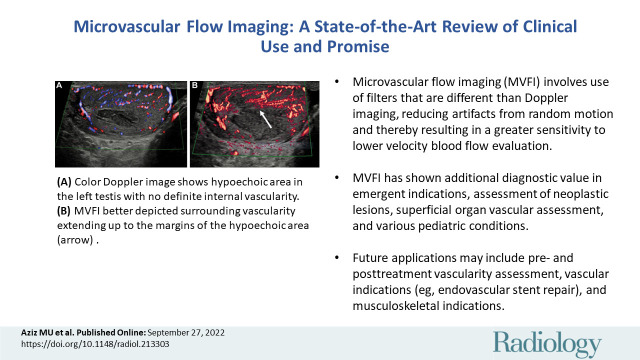
Microvascular Flow Imaging: A State-of-the-Art Review of Clinical Use and Promise
- PMID: 36165794
- PMCID: PMC9619200
- DOI: 10.1148/radiol.213303
Microvascular Flow Imaging: A State-of-the-Art Review of Clinical Use and Promise
Abstract
Vascular imaging with color and power Doppler is a useful tool in the assessment of various disease processes. Assessment of blood flow, from infarction and ischemia to hyperemia, in organs, neoplasms, and vessels, is used in nearly every US investigation. Recent developments in this area are sensitive to small-vessel low velocity flow without use of intravenous contrast agents, known as microvascular flow imaging (MVFI). MVFI is more sensitive in detection of small vessels than color, power, and spectral Doppler, reducing the need for follow-up contrast-enhanced US (CEUS), CT, and MRI, except when arterial and venous wash-in and washout characteristics would be helpful in diagnosis. Varying clinical applications of MVFI are reviewed in adult and pediatric populations, including its technical underpinnings. MVFI shows promise in assessment of several conditions including benign and malignant lesions in the liver and kidney, acute pathologic abnormalities in the gallbladder and testes, and superficial lymph nodes. Future potential of MVFI in different conditions (eg, endovascular repair) is discussed. Finally, clinical cases in which MVFI correlated and potentially obviated additional CEUS, CT, or MRI are shown.
© RSNA, 2022.
Conflict of interest statement
Figures
References
-
- Martinoli C , Derchi LE , Rizzatto G , Solbiati L . Power Doppler sonography: general principles, clinical applications, and future prospects . Eur Radiol 1998. ; 8 ( 7 ): 1224 – 1235 . - PubMed
-
- Cosgrove D , Lassau N . Imaging of perfusion using ultrasound . Eur J Nucl Med Mol Imaging 2010. ; 37 ( Suppl 1 ): S65 – S85 . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
