

Outcomes Associated With Timing of Neurologic Dysfunction Onset Relative to Pediatric Sepsis Recognition
- PMID: 36165937
- PMCID: PMC9524404
- DOI: 10.1097/PCC.0000000000002979
Outcomes Associated With Timing of Neurologic Dysfunction Onset Relative to Pediatric Sepsis Recognition
Abstract
Objectives: To compare outcomes associated with timing-early versus late-of any neurologic dysfunction during pediatric sepsis.
Design: Secondary analysis of a cross-sectional point prevalence study.
Setting: A total of 128 PICUs in 26 countries.
Patients: Less than 18 years with severe sepsis on 5 separate days (2013-2014).
Interventions: None.
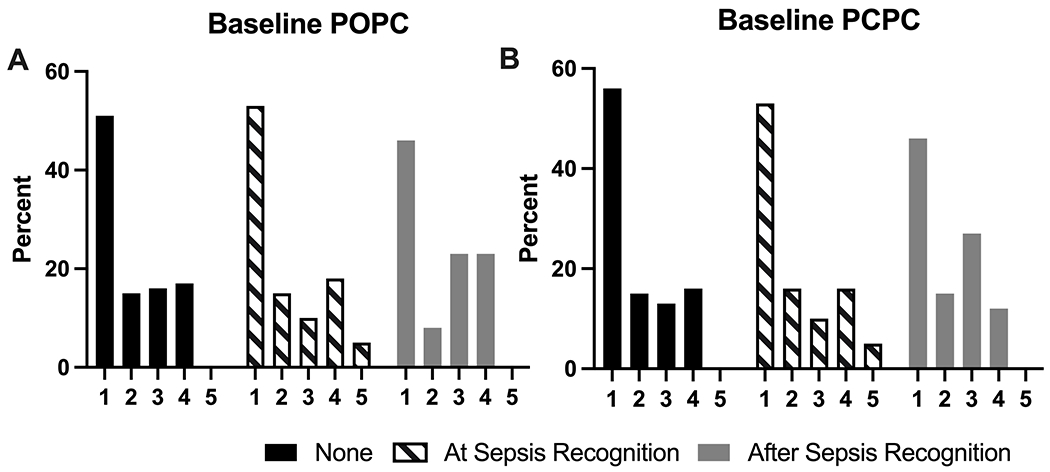
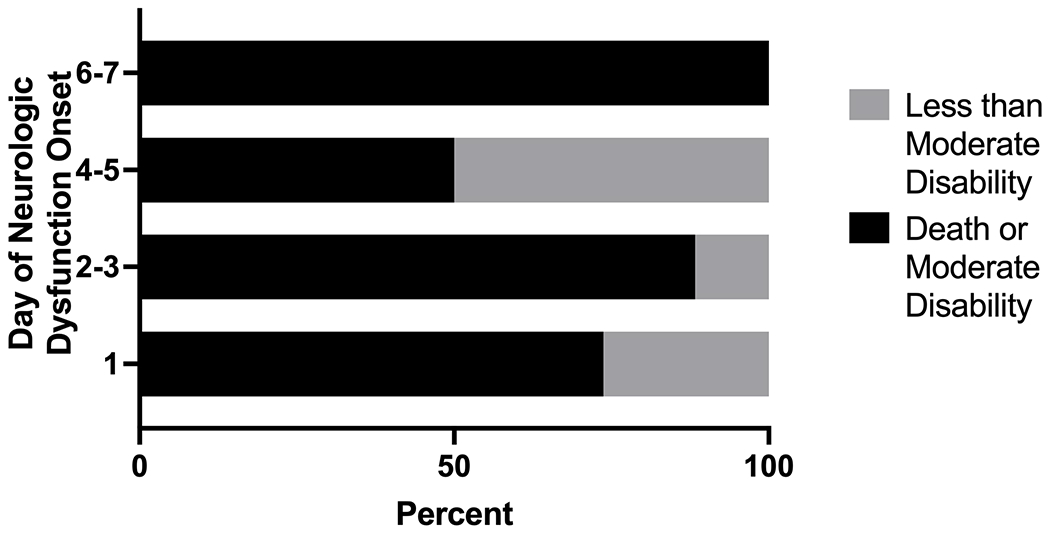
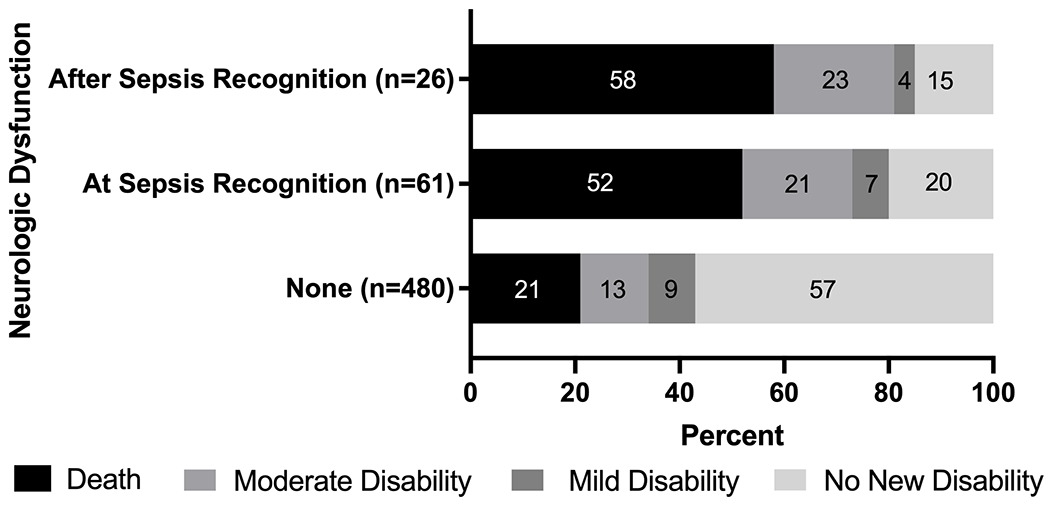
Measurements and main results: Patients were categorized as having either no neurologic dysfunction or neurologic dysfunction (i.e., present at or after sepsis recognition), which was defined as Glasgow Coma Scale score less than 5 and/or fixed dilated pupils. Our primary outcome was death or new moderate disability (i.e., Pediatric Overall [or Cerebral] Performance Category score ≥3 and change ≥1 from baseline) at hospital discharge, and 87 of 567 severe sepsis patients (15%) had neurologic dysfunction within 7 days of sepsis recognition (61 at sepsis recognition and 26 after sepsis recognition). Primary site of infection varied based on presence of neurologic dysfunction. Death or new moderate disability occurred in 161 of 480 (34%) without neurologic dysfunction, 45 of 61 (74%) with neurologic dysfunction at sepsis recognition, and 21 of 26 (81%) with neurologic dysfunction after sepsis recognition (p < 0.001 across all groups). On multivariable analysis, in comparison with those without neurologic dysfunction, neurologic dysfunction whether at sepsis recognition or after was associated with increased odds of death or new moderate disability (adjusted odds ratio, 4.9 [95% CI, 2.3-10.1] and 10.7 [95% CI, 3.8-30.5], respectively). We failed to identify a difference between these adjusted odds ratios of death or new moderate disability that would indicate a differential risk of outcome based on timing of neurologic dysfunction (p = 0.20).
Conclusions: In this severe sepsis international cohort, the presence of neurologic dysfunction during sepsis is associated with worse outcomes at hospital discharge. The impact of early versus late onset of neurologic dysfunction in sepsis on outcome remains unknown, and further work is needed to better understand timing of neurologic dysfunction onset in pediatric sepsis.
Copyright © 2022 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Drs. Weiss’ and Fitzgerald’s institutions received funding from Children’s Hospital of Philadelphia Center for Pediatric Clinical Effectiveness. Dr. Fitzgerald’s institution received funding from the National Institutes of Health (NIH). Dr. Loftis received support for article research from the NIH. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Late-Onset Neurologic Dysfunction in Pediatric Sepsis-What Brains Might Learn From Kidneys and Persistent Acute Kidney Injury.Pediatr Crit Care Med. 2022 Aug 1;23(8):659-661. doi: 10.1097/PCC.0000000000003007. Epub 2022 Aug 1. Pediatr Crit Care Med. 2022. PMID: 36165941 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
