

Peripheral Exudative Hemorrhagic Chorioretinopathy with and without treatment-Clinical and multimodal imaging characteristics and prognosis
- PMID: 36166419
- PMCID: PMC9514609
- DOI: 10.1371/journal.pone.0275163
Peripheral Exudative Hemorrhagic Chorioretinopathy with and without treatment-Clinical and multimodal imaging characteristics and prognosis
Abstract
Purpose: To describe clinical and imaging characteristics of patients with Peripheral Exudative Hemorrhagic Chorioretinopathy (PEHCR), prognosis and treatment response.
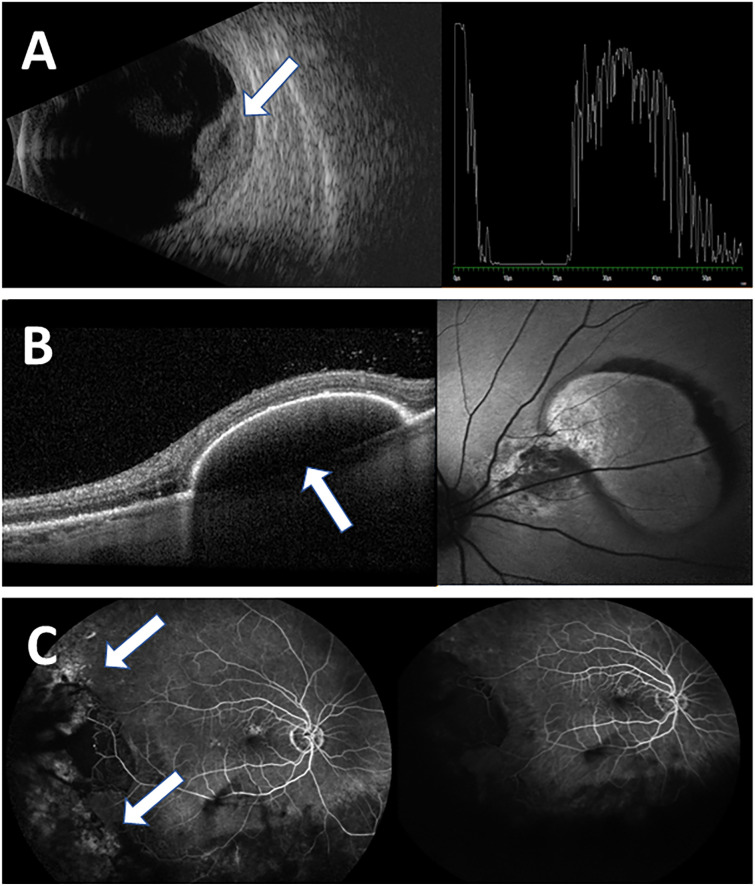
Methods: In this retrospective cohort study medical records of patients diagnosed with PEHCR in a tertiary medical center between 2008 and 2018 were reviewed. Collected data included demographics, medical history, ophthalmologic examination and multi-modal imaging including fundus autofluorescence, optical coherence tomography (OCT), ultrasound (US), fluorescein angiography and indocyanine green angiography when available. Bevacizumab treatment results were analyzed when applied.
Results: 35 eyes of 32 patients were included, with a female predominance (56.25%) and an average age of 79.0±9.87 years at presentation. Most common OCT and US findings were subretinal mass (68.75%), pigment epithelial detachment (30.00%) and atrophic changes (21.86%). Median follow-up period was 18.00 months (range 0-102). Visual acuity (VA) remained stable (39.29%) or improved (25.00%) in most cases available for follow-up. Treatment with intravitreal bevacizumab induced a statistically significant clinical resolution in 88.89% of eyes available for follow-up (8/9 eyes) (p = 0.02).
Conclusions: PEHCR is presented with high clinical variability and generally good prognosis. This is the first publication demonstrating a statistically significant clinical resolution of disease following intravitreal bevacizumab injections.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Kingham J.D (1978) Hemorrhagic detachment of the peripheral retinal pigment epithelium. Ann Ophthalmol, 1978. 10(2): p. 175–8. . - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
