

Healthcare resource utilization in patients with treatment-resistant depression-A Danish national registry study
- PMID: 36166443
- PMCID: PMC9514626
- DOI: 10.1371/journal.pone.0275299
Healthcare resource utilization in patients with treatment-resistant depression-A Danish national registry study
Abstract
Objectives: To investigate healthcare resource utilization (HRU) and associated costs by depression severity and year of diagnosis among patients with treatment-resistant depression (TRD) in Denmark.
Methods: Including all adult patients with a first-time hospital contact for major depressive disorder (MDD) in 1996-2015, TRD patients were defined at the second shift in depression treatment (antidepressant medicine or electroconvulsive therapy) and matched 1:2 with non-TRD patients. The risk of utilization and amount of HRU and associated costs including medicine expenses 12 months after the TRD-defining date were reported, comparing TRD patients with non-TRD MDD patients.
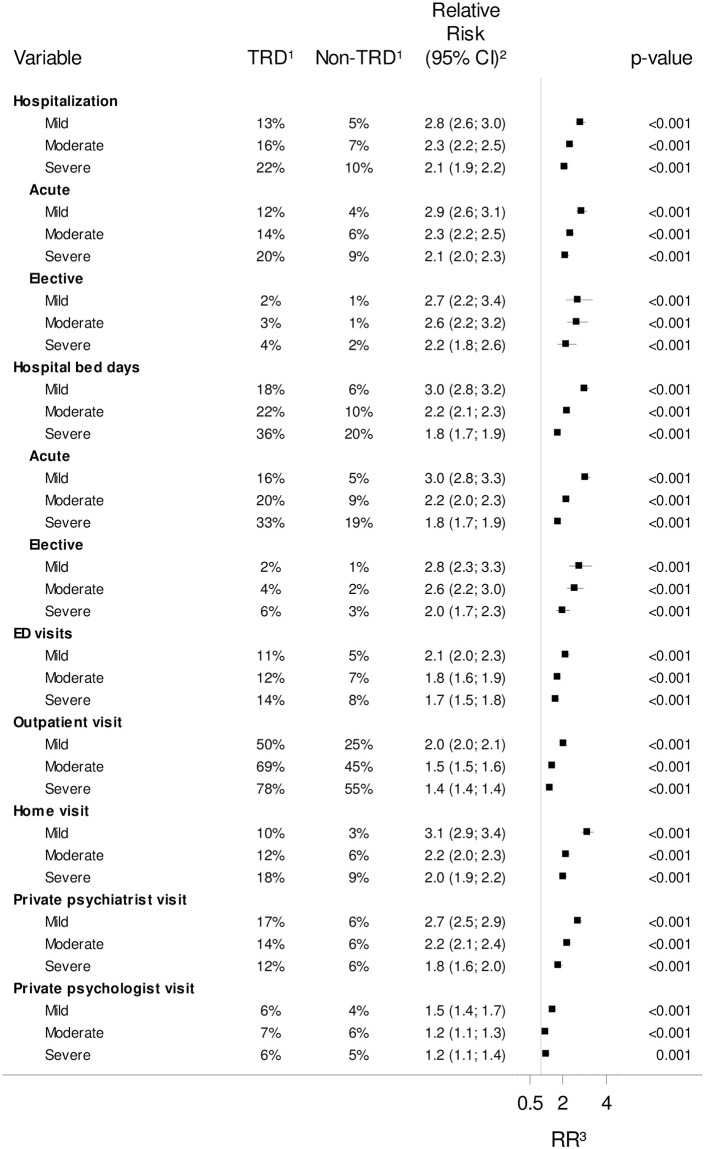
Results: Identifying 25,321 TRD-patients matched with 50,638 non-TRD patients, the risk of psychiatric hospitalization following TRD diagnosis was 138.4% (95%-confidence interval: 128.3-149.0) higher for TRD patients than for non-TRD MDD patients. The number of hospital bed days and emergency department (ED) visits were also higher among TRD patients, with no significant difference for somatic HRU. Among patients who incurred healthcare costs, the associated HRU costs for TRD patients were 101.9% (97.5-106.4) higher overall, and 55.2% (50.9-59.6) higher for psychiatric services than those of non-TRD patients. The relative differences in costs for TRD-patients vs non-TRD patients were greater for patients with mild depression and tended to increase over the study period (1996-2015), particularly for acute hospitalizations and ED visits.
Limitations: TRD was defined by prescription patterns besides ECT treatments.
Conclusion: TRD was associated with increased psychiatric-related HRU. Particularly the difference in acute hospitalizations and ED visits between TRD and non-TRD patients increased over the study period.
Conflict of interest statement
The study was performed by the Copenhagen Phase IV Unit (Phase4CPH) and was financed by Janssen Cilag A/S, which holds license to antidepressant medicine. Via Phase4CPH, JP, EJS and MZA have performed other studies regarding antidepressants involving funding from Janssen Cilag and Eli Lilly, while KJJ, FHG and MO have performed other studies regarding antidepressants involving funding from Janssen Cilag. All funds were given to their institution. JR, NB and SA are employees of Janssen Cilag. Janssen Cilag A/S and its employees did not have access to the registry data located on the servers of Statistics Denmark and had therefore no influence on the data management and data analysis of the present work. The authors at Copenhagen Phase IV Unit retained editorial control of the manuscript. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures


References
-
- World Health Organization. Depression and Other Common Mental Disorders—Global Health Estimates. World Health Organization 2017; 2017. https://www.who.int/mental_health/management/depression/prevalence_globa...
-
- Alonso J, Angermeyer MC, Bernert S, Bruffaerts R, Brugha TS, Bryson H, et al. Prevalence of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand Suppl. 2004; 21–27. doi: 10.1111/j.1600-0047.2004.00327.x - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
