

NASH and Hepatocellular Carcinoma: Immunology and Immunotherapy
- PMID: 36166660
- PMCID: PMC9890137
- DOI: 10.1158/1078-0432.CCR-21-1258
NASH and Hepatocellular Carcinoma: Immunology and Immunotherapy
Abstract
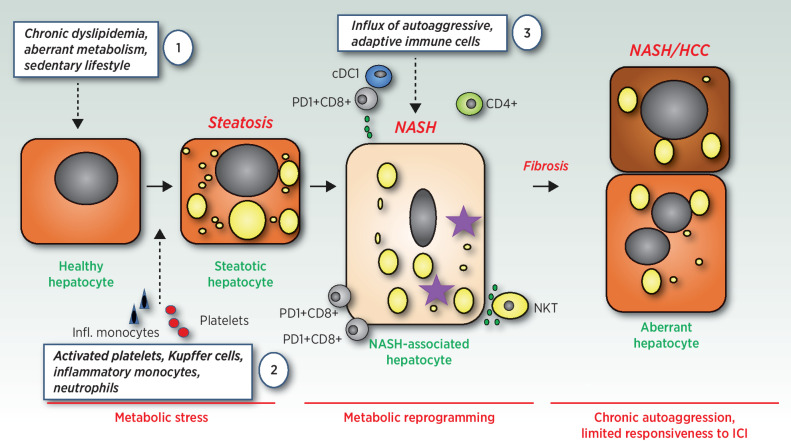
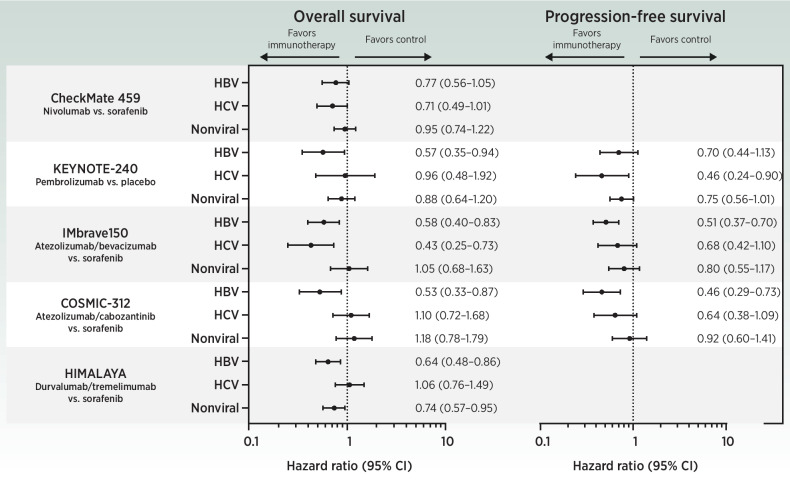
The last 10 years have revolutionized our basic understanding of nonalcoholic fatty liver disease and consequent liver cancer. It has become clear that several innate and adaptive immune cells play an important role in initiating, maintaining, or exacerbating nonalcoholic steatohepatitis (NASH)-a disease that has been recently defined as autoaggressive. Despite improved disease management aimed at reducing the progression of fibrosis, NASH is set to become a leading cause for hepatocellular carcinoma (HCC). Preliminary data from preclinical studies suggest that immunotherapy efficacy may be reduced in NASH-related HCC compared with viral HCC; however, conclusive evidence supporting clinical translation of these findings is lacking. Comprehensive clinical and immunologic phenotyping of mechanisms linking NASH progression with carcinogenesis and therapeutic resistance is key to prevent progression to cirrhosis, improve monitoring and stratification of NASH according to predicted cancer risk, and ultimately increase survival of patients with NASH-HCC. In this review, we summarize the state of the art in the field of NASH and NASH-HCC with focus on immunobiology. We discuss preclinical and clinical findings underpinning NASH as an immunologically distinct pro-tumorigenic disease entity, and explore areas of potential therapeutic vulnerabilities in NASH-associated HCC.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, et al. . Global burden of NAFLD and NASH: trends, predictions, risk factors, and prevention. Nat Rev Gastroenterol Hepatol 2018;15:11–20. - PubMed
-
- Villanueva A. Hepatocellular carcinoma. N Engl J Med 2019;380:1450–62. - PubMed
-
- Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, et al. . Hepatocellular carcinoma. Nat Rev Dis Primers 2021;7:6. - PubMed
-
- Gehrke N, Schattenberg JM. Metabolic inflammation—a role for hepatic inflammatory pathways as drivers of comorbidities in nonalcoholic fatty liver disease? Gastroenterology 2020;158:1929–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
