

The association between TMAO, CMPF, and clinical outcomes in advanced chronic kidney disease: results from the European QUALity (EQUAL) Study
- PMID: 36166845
- PMCID: PMC9761748
- DOI: 10.1093/ajcn/nqac278
The association between TMAO, CMPF, and clinical outcomes in advanced chronic kidney disease: results from the European QUALity (EQUAL) Study
Abstract
Background: Trimethylamine N-oxide (TMAO), a metabolite from red meat and fish consumption, plays a role in promoting cardiovascular events. However, data regarding TMAO and its impact on clinical outcomes are inconclusive, possibly due to its undetermined dietary source.
Objectives: We hypothesized that circulating TMAO derived from fish intake might cause less harm compared with red meat sources by examining the concomitant level of 3-carboxy-4-methyl-5-propyl-2-furanpropionate (CMPF), a known biomarker of fish intake, and investigated the association between TMAO, CMPF, and outcomes.
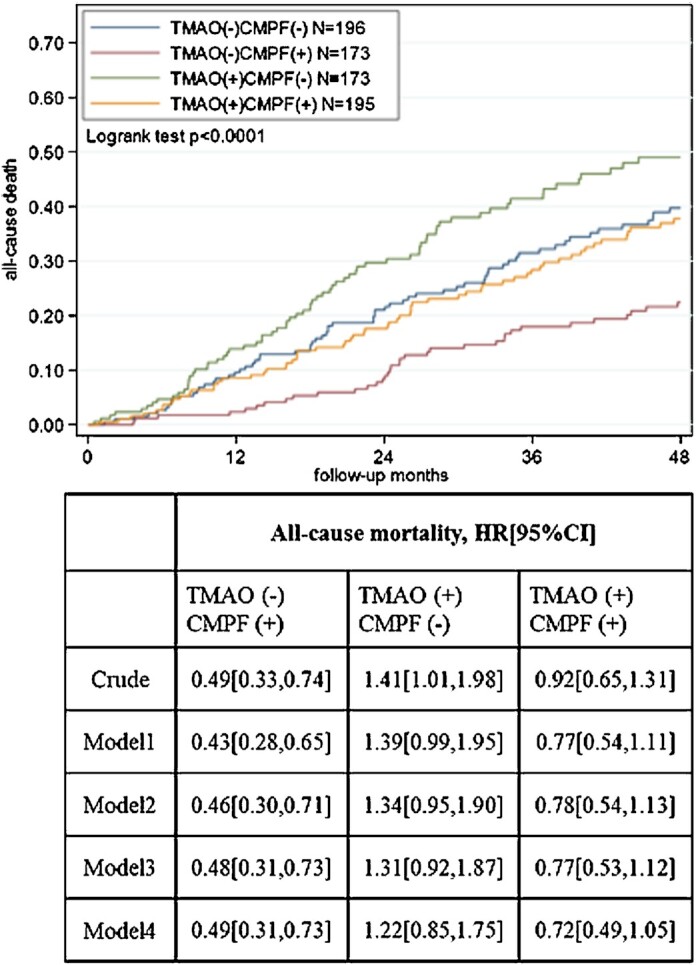
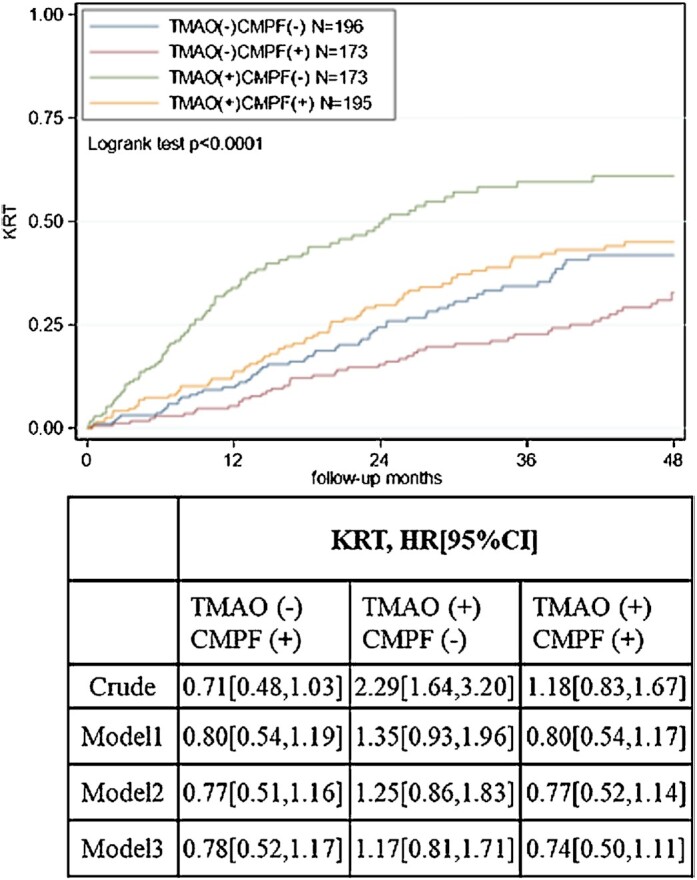
Methods: Patients were recruited from the European QUALity (EQUAL) Study on treatment in advanced chronic kidney disease among individuals aged ≥65 y whose estimated glomerular filtration rate (eGFR) had dropped for the first time to ≤20 mL/min per 1.73 m2 during the last 6 mo. The association between TMAO, CMPF, and outcomes including all-cause mortality and kidney replacement therapy (KRT) was assessed among 737 patients. Patients were further stratified by median cutoffs of TMAO and CMPF, suggesting high/low red meat and fish intake.
Results: During a median of 39 mo of follow-up, 232 patients died. Higher TMAO was independently associated with an increased risk of all-cause mortality (multivariable HR: 1.46; 95% CI: 1.17, 1.83). Higher CMPF was associated with a reduced risk of both all-cause mortality (HR: 0.79; 95% CI: 0.71, 0.89) and KRT (HR: 0.80; 95% CI: 0.71, 0.90), independently of TMAO and other clinically relevant confounders. In comparison to patients with low TMAO and CMPF, patients with low TMAO and high CMPF had reduced risk of all-cause mortality (adjusted HR: 0.49; 95% CI: 0.31, 0.73), whereas those with high TMAO and high CMPF showed no association across adjusted models.
Conclusions: High CMPF conferred an independent role in health benefits and might even counteract the unfavorable association between TMAO and outcomes. Whether higher circulating CMPF concentrations are due to fish consumption, and/or if CMPF is a protective factor, remains to be verified.
Keywords: 3-carboxy-4-methyl-5-propyl-2-furanpropionate; CKD; fish intake; kidney replacement therapy; mortality; red meat; trimethylamine N-oxide; uremic toxins.
© The Author(s) 2022. Published by Oxford University Press on behalf of the American Society for Nutrition.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu C. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296–305. - PubMed
-
- Kalantar-Zadeh K, Block G, Humphreys MH, Kopple JD. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int. 2003;63(3):793–808. - PubMed
-
- Elliott MK, McCaughan JA, Fogarty DG. Do patients with chronic kidney disease get optimal cardiovascular risk reduction?. Curr Opin Nephrol Hypertens. 2014;23(3):267–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
