

GD2-targeting CAR-T cells enhanced by transgenic IL-15 expression are an effective and clinically feasible therapy for glioblastoma
- PMID: 36167468
- PMCID: PMC9516307
- DOI: 10.1136/jitc-2022-005187
GD2-targeting CAR-T cells enhanced by transgenic IL-15 expression are an effective and clinically feasible therapy for glioblastoma
Abstract
Background: Aggressive primary brain tumors such as glioblastoma are uniquely challenging to treat. The intracranial location poses barriers to therapy, and the potential for severe toxicity. Effective treatments for primary brain tumors are limited, and 5-year survival rates remain poor. Immune checkpoint inhibitor therapy has transformed treatment of some other cancers but has yet to significantly benefit patients with glioblastoma. Early phase trials of chimeric antigen receptor (CAR) T-cell therapy in patients with glioblastoma have demonstrated that this approach is safe and feasible, but with limited evidence of its effectiveness. The choices of appropriate target antigens for CAR-T-cell therapy also remain limited.
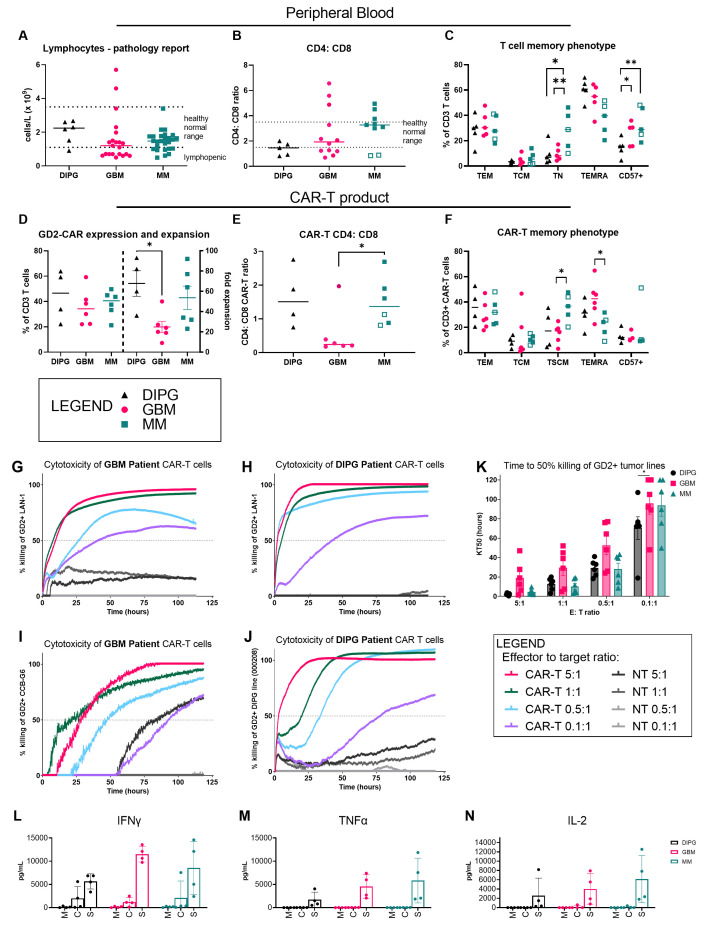
Methods: We profiled an extensive biobank of patients' biopsy tissues and patient-derived early passage glioma neural stem cell lines for GD2 expression using immunomicroscopy and flow cytometry. We then employed an approved clinical manufacturing process to make CAR- T cells from patients with peripheral blood of glioblastoma and diffuse midline glioma and characterized their phenotype and function in vitro. Finally, we tested intravenously administered CAR-T cells in an aggressive intracranial xenograft model of glioblastoma and used multicolor flow cytometry, multicolor whole-tissue immunofluorescence and next-generation RNA sequencing to uncover markers associated with effective tumor control.
Results: Here we show that the tumor-associated antigen GD2 is highly and consistently expressed in primary glioblastoma tissue removed at surgery. Moreover, despite patients with glioblastoma having perturbations in their immune system, highly functional GD2-specific CAR-T cells can be produced from their peripheral T cells using an approved clinical manufacturing process. Finally, after intravenous administration, GD2-CAR-T cells effectively infiltrated the brain and controlled tumor growth in an aggressive orthotopic xenograft model of glioblastoma. Tumor control was further improved using CAR-T cells manufactured with a clinical retroviral vector encoding an interleukin-15 transgene alongside the GD2-specific CAR. These CAR-T cells achieved a striking 50% complete response rate by bioluminescence imaging in established intracranial tumors.
Conclusions: Targeting GD2 using a clinically deployed CAR-T-cell therapy has a sound scientific and clinical rationale as a treatment for glioblastoma and other aggressive primary brain tumors.
Keywords: brain neoplasms; immunotherapy, adoptive; receptors, chimeric antigen.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical