

Comparison of single-shot EPI and multi-shot EPI in prostate DWI at 3.0 T
- PMID: 36168032
- PMCID: PMC9515065
- DOI: 10.1038/s41598-022-20518-8
Comparison of single-shot EPI and multi-shot EPI in prostate DWI at 3.0 T
Abstract
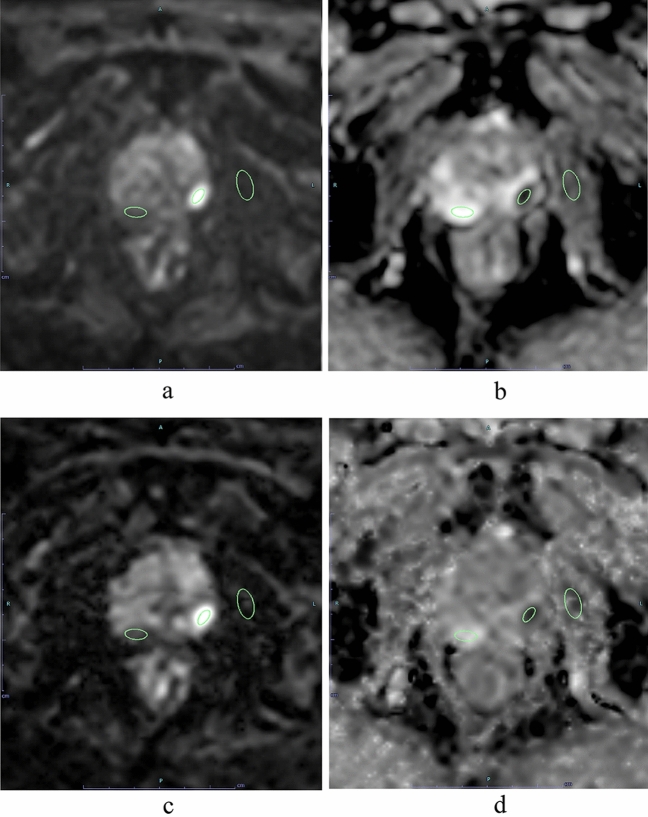
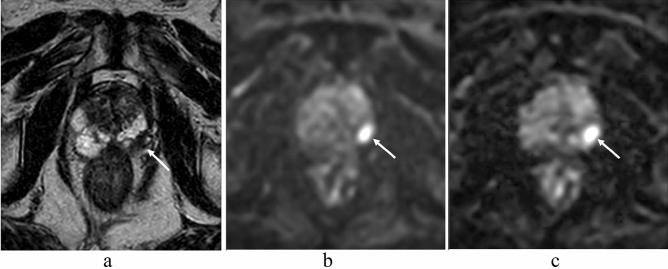
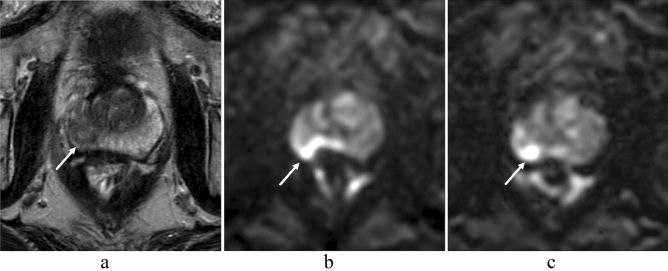
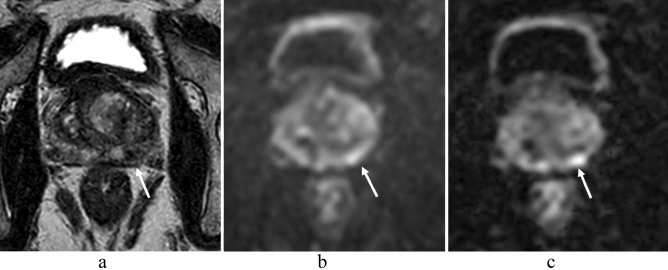
In prostate MRI, single-shot EPI (ssEPI) DWI still suffers from distortion and blurring. Multi-shot EPI (msEPI) overcomes the drawbacks of ssEPI DWI. The aim of this article was to compare the image quality and diagnostic performance for clinically significant prostate cancer (csPC) between ssEPI DWI and msEPI DWI. This retrospective study included 134 patients with suspected PC who underwent 3.0 T MRI and subsequent MRI-guided biopsy. Three radiologists independently assessed anatomical distortion, prostate edge clarity, and lesion conspicuity score for pathologically confirmed csPC. Lesion apparent diffusion coefficient (ADC) and benign ADC were also calculated. In 17 PC patients who underwent prostatectomy, three radiologists independently assessed eight prostate regions by DWI score in PI-RADS v 2.1. Anatomical distortion and prostate edge clarity were significantly higher in msEPI DWI than in ssEPI DWI in the three readers. Lesion conspicuity score was significantly higher in msEPI DWI than in ssEPI DWI in reader 1 and reader 3. Regarding discrimination ability between PC with GS ≤ 3 + 4 and PC with GS ≥ 4 + 3 using lesion ADC, AUC was comparable between ssEPI DWI and msEPI DWI. For diagnostic performance of csPC using DWI score, AUC was comparable between msEPI DWI and ssEPI DWI in all readers. Compared with ssEPI DWI, msEPI DWI had improved image quality and similar or higher diagnostic performance.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Reduced field-of-view and multi-shot DWI acquisition techniques: Prospective evaluation of image quality and distortion reduction in prostate cancer imaging.Magn Reson Imaging. 2022 Nov;93:108-114. doi: 10.1016/j.mri.2022.08.008. Epub 2022 Aug 6. Magn Reson Imaging. 2022. PMID: 35944809 Free PMC article.
-
Comparison of single shot and multishot diffusion-weighted imaging in 5-T magnetic resonance imaging for brain disease diagnosis.Quant Imaging Med Surg. 2024 Oct 1;14(10):7291-7305. doi: 10.21037/qims-24-118. Epub 2024 Sep 26. Quant Imaging Med Surg. 2024. PMID: 39429579 Free PMC article.
-
Applicability of readout-segmented echoplanar diffusion weighted imaging for prostate MRI.Medicine (Baltimore). 2019 Jul;98(29):e16447. doi: 10.1097/MD.0000000000016447. Medicine (Baltimore). 2019. PMID: 31335699 Free PMC article.
-
Multiparametric MRI in detection and staging of prostate cancer.Dan Med J. 2017 Feb;64(2):B5327. Dan Med J. 2017. PMID: 28157066 Review.
-
Diffusion-weighted imaging in prostate cancer.MAGMA. 2022 Aug;35(4):533-547. doi: 10.1007/s10334-021-00957-6. Epub 2021 Sep 7. MAGMA. 2022. PMID: 34491467 Review.
Cited by
-
Comparison of readout-segmented echo-planar imaging and single-shot echo-planar imaging in the fetal brain.Transl Pediatr. 2025 May 30;14(5):844-854. doi: 10.21037/tp-2025-77. Epub 2025 May 27. Transl Pediatr. 2025. PMID: 40519742 Free PMC article.
-
Multiparametric Magnetic Resonance Imaging of Penile Cancer: A Pictorial Review.Cancers (Basel). 2023 Nov 8;15(22):5324. doi: 10.3390/cancers15225324. Cancers (Basel). 2023. PMID: 38001583 Free PMC article. Review.
-
Advancements in Diffusion MRI Tractography for Neurosurgery.Invest Radiol. 2024 Jan 1;59(1):13-25. doi: 10.1097/RLI.0000000000001015. Epub 2023 Sep 14. Invest Radiol. 2024. PMID: 37707839 Free PMC article.
-
Comparative analysis of image quality and diagnostic performance among SS-EPI, MS-EPI, and rFOV DWI in bladder cancer.Jpn J Radiol. 2025 Apr;43(4):666-675. doi: 10.1007/s11604-024-01694-1. Epub 2024 Nov 16. Jpn J Radiol. 2025. PMID: 39548050 Free PMC article.
-
Convolutional network denoising for acceleration of multi-shot diffusion MRI.Magn Reson Imaging. 2024 Jan;105:108-113. doi: 10.1016/j.mri.2023.10.002. Epub 2023 Nov 19. Magn Reson Imaging. 2024. PMID: 37820978 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
