

Improving antimicrobial prescribing for upper respiratory infections in the emergency department: Implementation of peer comparison with behavioral feedback
- PMID: 36168488
- PMCID: PMC9495637
- DOI: 10.1017/ash.2021.240
Improving antimicrobial prescribing for upper respiratory infections in the emergency department: Implementation of peer comparison with behavioral feedback
Abstract
Objective: To reduce inappropriate antibiotic prescribing for acute respiratory infections (ARIs) by employing peer comparison with behavioral feedback in the emergency department (ED).
Design: A controlled before-and-after study.
Setting: The study was conducted in 5 adult EDs at teaching and community hospitals in a health system.
Patients: Adults presenting to the ED with a respiratory condition diagnosis code. Hospitalized patients and those with a diagnosis code for a non-respiratory condition for which antibiotics are or may be warranted were excluded.
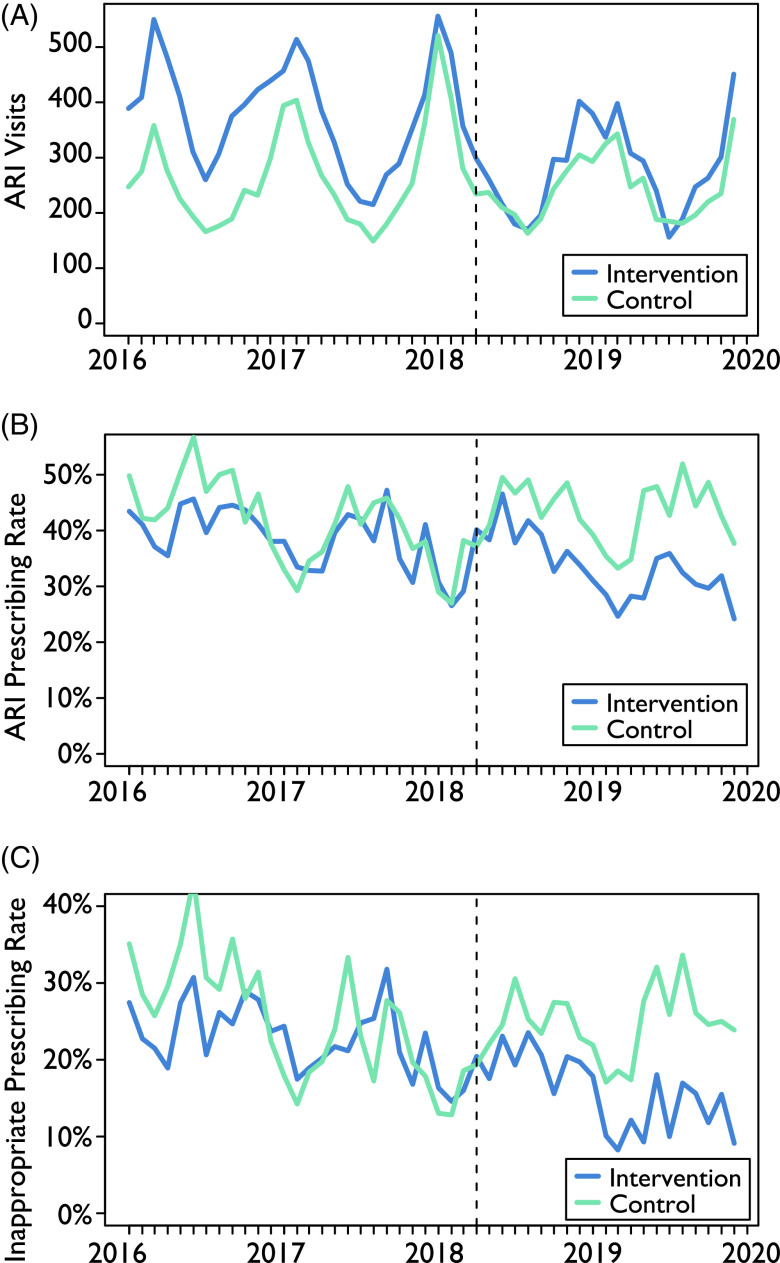
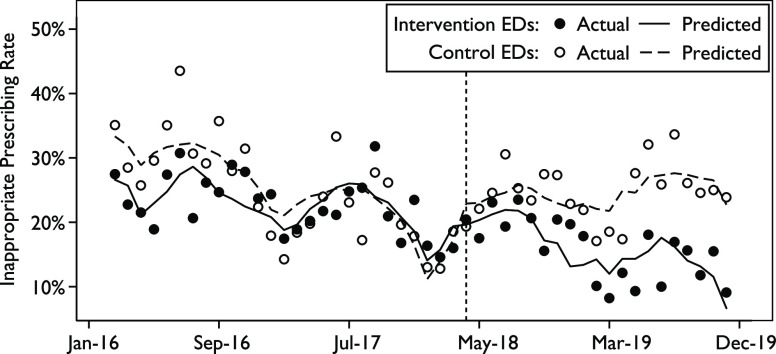
Interventions: After a baseline period from January 2016 to March 2018, 3 EDs implemented a feedback intervention with peer comparison between April 2018 and December 2019 for attending physicians. Also, 2 EDs in the health system served as controls. Using interrupted time series analysis, the inappropriate ARI prescribing rate was calculated as the proportion of antibiotic-inappropriate ARI encounters with a prescription. Prescribing rates were also evaluated for all ARIs. Attending physicians at intervention sites received biannual e-mails with their inappropriate prescribing rate and had access to a dashboard that was updated daily showing their performance relative to their peers.
Results: Among 28,544 ARI encounters, the inappropriate prescribing rate remained stable at the control EDs between the 2 periods (23.0% and 23.8%). At the intervention sites, the inappropriate prescribing rate decreased significantly from 22.0% to 15.2%. Between periods, the overall ARI prescribing rate was 38.1% and 40.6% in the control group and 35.9% and 30.6% in the intervention group.
Conclusions: Behavioral feedback with peer comparison can be implemented effectively in the ED to reduce inappropriate prescribing for ARIs.
© The Author(s) 2021.
Figures
Similar articles
-
Use of behavioral economics and social psychology to improve treatment of acute respiratory infections (BEARI): rationale and design of a cluster randomized controlled trial [1RC4AG039115-01]--study protocol and baseline practice and provider characteristics.BMC Infect Dis. 2013 Jun 27;13:290. doi: 10.1186/1471-2334-13-290. BMC Infect Dis. 2013. PMID: 23806017 Free PMC article. Clinical Trial.
-
Behavioral interventions to reduce inappropriate antibiotic prescribing: a randomized pilot trial.BMC Infect Dis. 2016 Aug 5;16:373. doi: 10.1186/s12879-016-1715-8. BMC Infect Dis. 2016. PMID: 27495917 Free PMC article. Clinical Trial.
-
Using Audit and Feedback to Improve Antimicrobial Prescribing in Emergency Departments: A Multicenter Quasi-Experimental Study in the Veterans Health Administration.Open Forum Infect Dis. 2021 Apr 14;8(6):ofab186. doi: 10.1093/ofid/ofab186. eCollection 2021 Jun. Open Forum Infect Dis. 2021. PMID: 34113685 Free PMC article.
-
Effect of Behavioral Interventions on Inappropriate Antibiotic Prescribing Among Primary Care Practices: A Randomized Clinical Trial.JAMA. 2016 Feb 9;315(6):562-70. doi: 10.1001/jama.2016.0275. JAMA. 2016. PMID: 26864410 Free PMC article. Clinical Trial.
-
Prevalence and healthcare burden of inappropriate antimicrobial treatment in patients at high risk of complications from acute respiratory infections: a scoping review.Front Med (Lausanne). 2025 May 16;12:1533797. doi: 10.3389/fmed.2025.1533797. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40454140 Free PMC article.
Cited by
-
Development of a Reference Standard to Assign Bacterial Versus Viral Infection Etiology Using an All-inclusive Methodology for Comparison of Novel Diagnostic Tool Performance.Clin Infect Dis. 2025 Apr 30;80(4):735-743. doi: 10.1093/cid/ciae656. Clin Infect Dis. 2025. PMID: 39750735 Free PMC article.
-
The Effectiveness of Interactive Dashboards to Optimise Antibiotic Prescribing in Primary Care: A Systematic Review.Antibiotics (Basel). 2023 Jan 10;12(1):136. doi: 10.3390/antibiotics12010136. Antibiotics (Basel). 2023. PMID: 36671337 Free PMC article. Review.
References
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016;315:1864. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous