

Feasibility of implementing a telephone-based frailty assessment
- PMID: 36169216
- PMCID: PMC9772097
- DOI: 10.1111/jgs.18031
Feasibility of implementing a telephone-based frailty assessment
Abstract
Background: Despite the growing literature on the importance of identifying and managing frailty, its assessment has been limited in clinical settings. With the goal of integrating frailty assessment into routine clinical practice, this quality improvement project aimed to determine the feasibility, acceptability, and utility of administering a telephone-based frailty assessment.
Methods: Between 9/2020 and 6/2021, we identified 169 established patients with serious illnesses in an academic primary care-geriatric clinic. Patients were contacted via telephone, and their current medical, functional, nutritional, cognitive, and mood statuses were assessed using validated screening tools. A deficit-accumulation frailty score was then calculated using an electronic medical record-based frailty index calculator and standardized documentation with recommendations was generated for providers. The primary outcome was feasibility, measured as the proportion of patients successfully assessed. Secondary outcomes included completion rates of each domain, administration time, providers' perception, and clinical utility of the assessment.
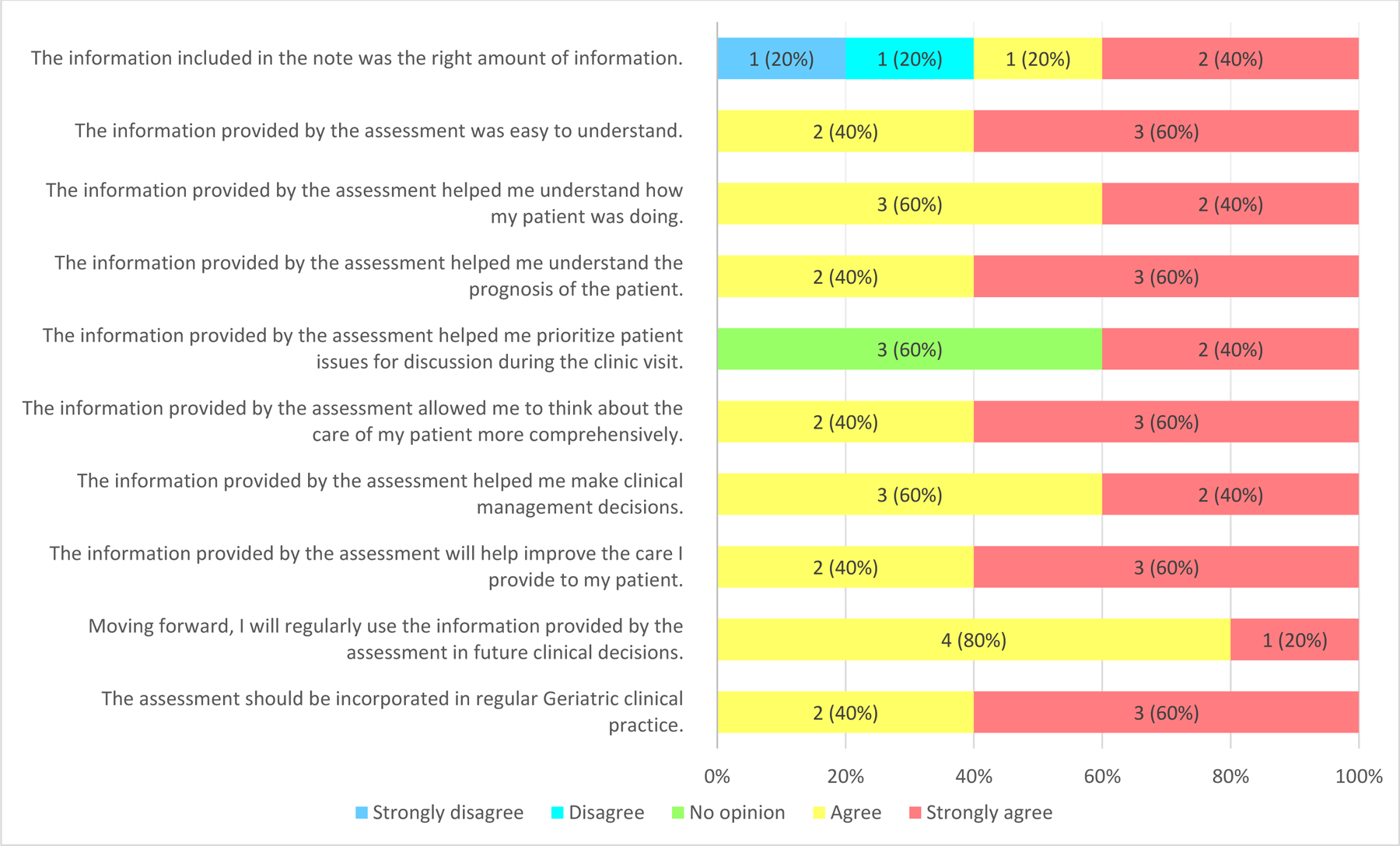
Results: A total of 139 (82.2%) patients, mean age of 82 years, 63.3% frail were successfully assessed. Of the 139 assessments, medical and functional domains were completed for all, while nutrition, mood, and cognition were completed by 88.5% (n = 123), 68.3% (n = 95), and 59.7% (n = 83) of the time, respectively. Conducting the full assessment took an average (standard deviation) time of 26.1 (7.3) minutes. Without the cognitive and mood domain, assessment took an average of 15.7 (7.5) minutes. Patients' providers found the information from the assessment helpful in evaluating and managing their patients. Care plans of 51.8% and 65.0% of patients who had mobility and mind issues, respectively, addressed these domains within 30 days after the assessment.
Conclusion: Implementation of the telephone-based frailty assessment is feasible, acceptable, and has the potential to influence the care plans of older adults. This work demonstrated how frailty assessment can be integrated with the outpatient setting.
Keywords: feasibility; implementation; multidomain assessment; outpatient.
© 2022 The American Geriatrics Society.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
