

Early vs Late Surgical Decompression for Central Cord Syndrome
- PMID: 36169962
- PMCID: PMC9520438
- DOI: 10.1001/jamasurg.2022.4454
Early vs Late Surgical Decompression for Central Cord Syndrome
Abstract
Importance: The optimal clinical management of central cord syndrome (CCS) remains unclear; yet this is becoming an increasingly relevant public health problem in the face of an aging population.
Objective: To provide a head-to-head comparison of the neurologic and functional outcomes of early (<24 hours) vs late (≥24 hours) surgical decompression for CCS.
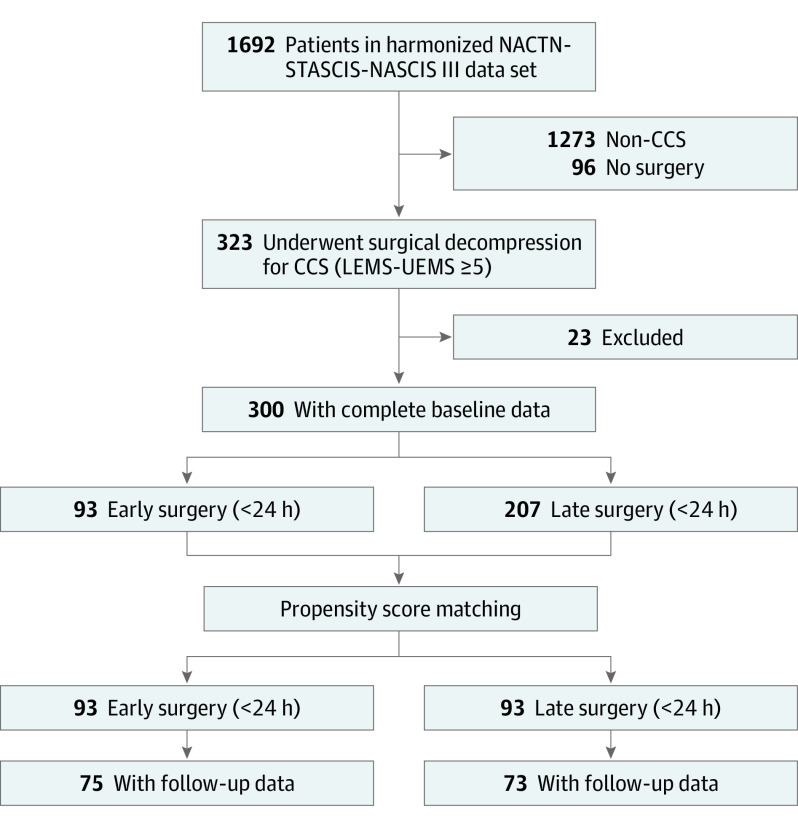
Design, setting, and participants: Patients who underwent surgery for CCS (lower extremity motor score [LEMS] - upper extremity motor score [UEMS] ≥ 5) were included in this propensity score-matched cohort study. Data were collected from December 1991 to March 2017, and the analysis was performed from March 2020 to January 2021. This study identified patients with CCS from 3 international multicenter studies with data on the timing of surgical decompression in spinal cord injury. Participants were included if they had a documented baseline neurologic examination performed within 14 days of injury. Participants were eligible if they underwent surgical decompression for CCS.
Exposures: Early surgery was compared with late surgery.
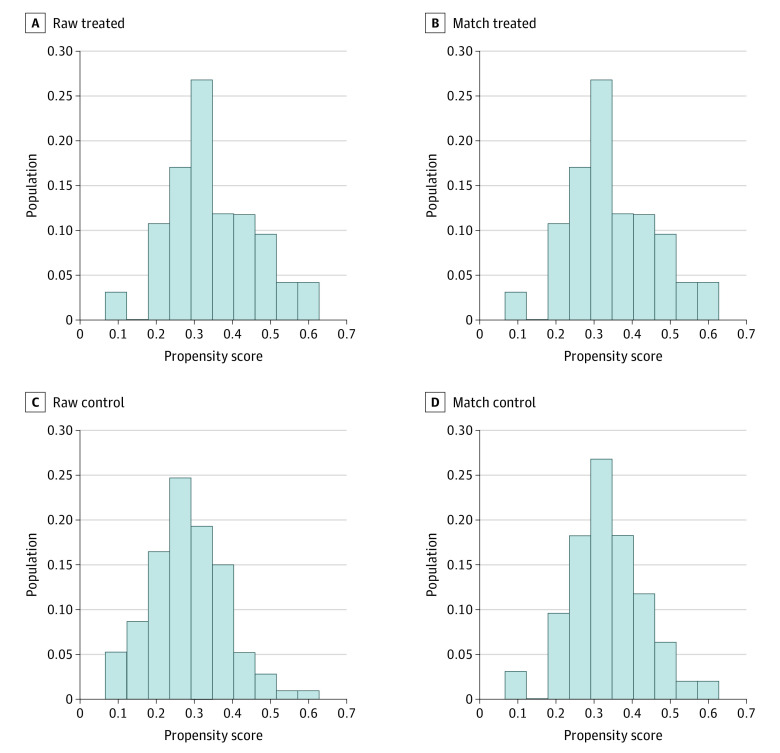
Main outcomes and measures: Propensity scores were calculated as the probability of undergoing early compared with late surgery using the logit method and adjusting for relevant confounders. Propensity score matching was performed in a 1:1 ratio by an optimal-matching technique. The primary end point was motor recovery (UEMS, LEMS, American Spinal Injury Association [ASIA] motor score [AMS]) at 1 year. Secondary end points were Functional Independence Measure (FIM) motor score and complete independence in each FIM motor domain at 1 year.
Results: The final study cohort consisted of 186 patients with CCS. The early-surgery group included 93 patients (mean [SD] age, 47.8 [16.8] years; 66 male [71.0%]), and the late-surgery group included 93 patients (mean [SD] age, 48.0 [15.5] years; 75 male [80.6%]). Early surgical decompression resulted in significantly improved recovery in upper limb (mean difference [MD], 2.3; 95% CI, 0-4.5; P = .047), but not lower limb (MD, 1.1; 95% CI, -0.8 to 3.0; P = .30), motor function. In an a priori-planned subgroup analysis, outcomes were comparable with early or late decompressive surgery in patients with ASIA Impairment Scale (AIS) grade D injury. However, in patients with AIS grade C injury, early surgery resulted in significantly greater recovery in overall motor score (MD, 9.5; 95% CI, 0.5-18.4; P = .04), owing to gains in both upper and lower limb motor function.
Conclusions and relevance: This cohort study found early surgical decompression to be associated with improved recovery in upper limb motor function at 1 year in patients with CCS. Treatment paradigms for CCS should be redefined to encompass early surgical decompression as a neuroprotective therapy.
Conflict of interest statement
Figures
Comment on
-
Central Cord Syndrome Is Likewise a Surgical Emergency-Time Is Spine.JAMA Surg. 2022 Nov 1;157(11):1032-1033. doi: 10.1001/jamasurg.2022.4455. JAMA Surg. 2022. PMID: 36169970 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
