

Evaluation of outcome from endovascular therapy for Budd-Chiari syndrome: a systematic review and meta-analysis
- PMID: 36171454
- PMCID: PMC9519873
- DOI: 10.1038/s41598-022-20399-x
Evaluation of outcome from endovascular therapy for Budd-Chiari syndrome: a systematic review and meta-analysis
Abstract
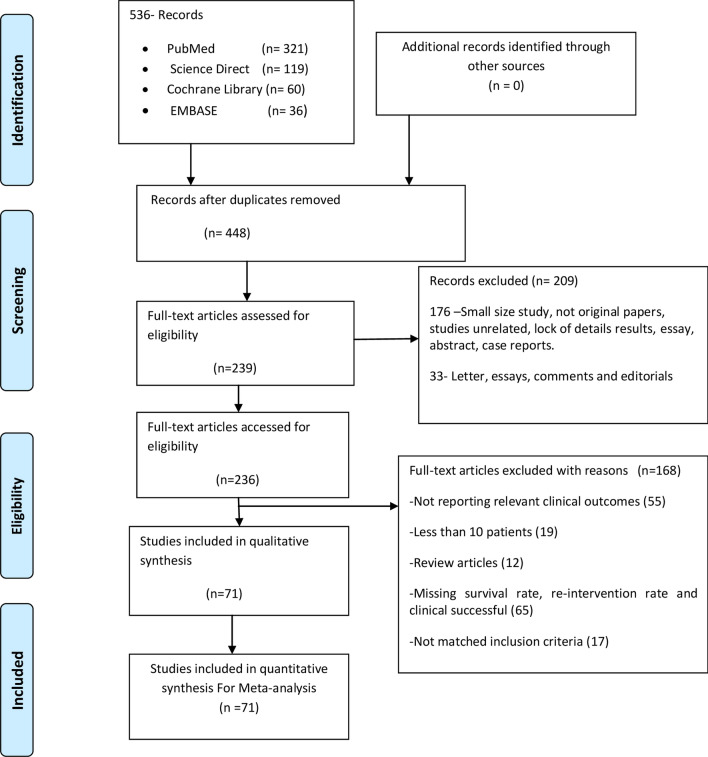
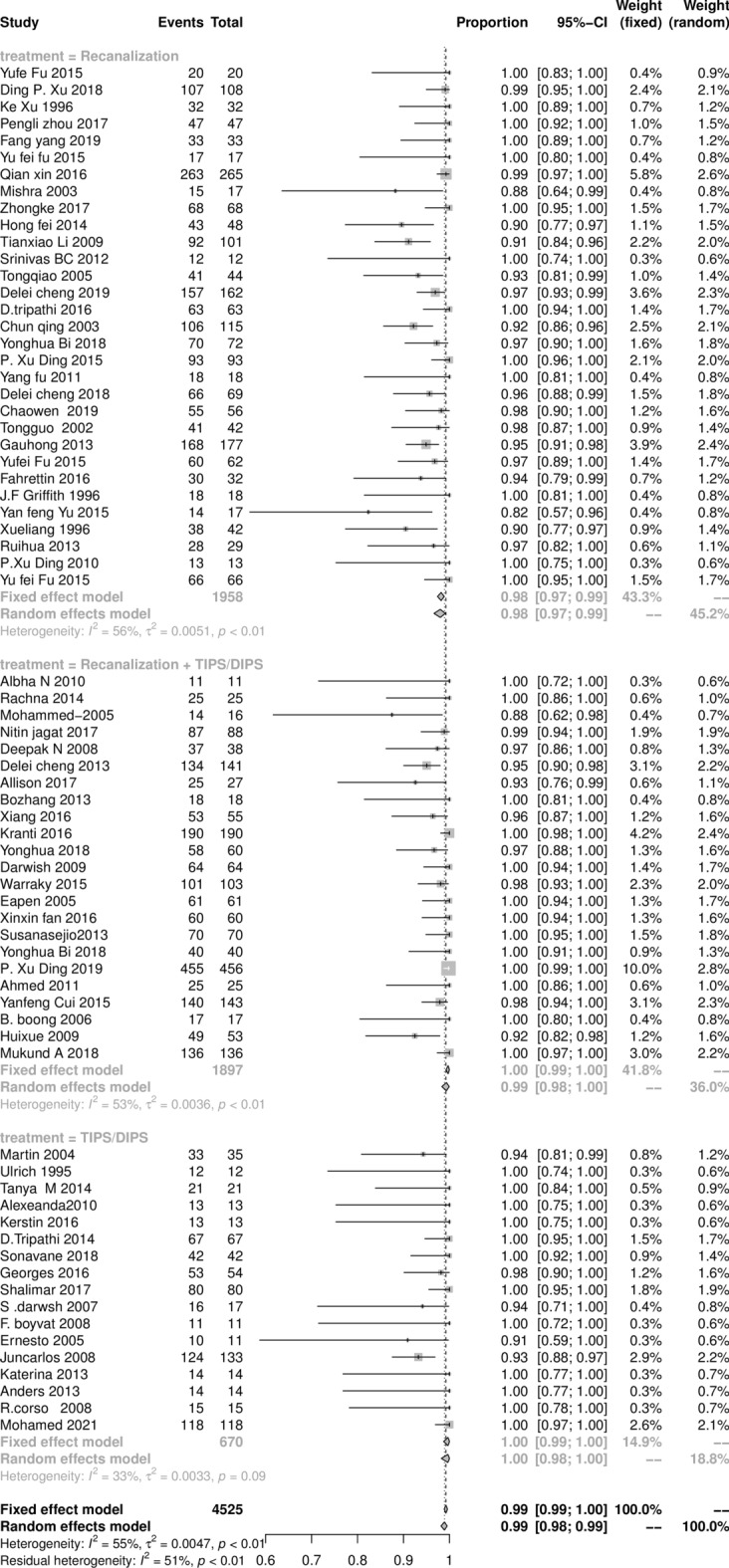
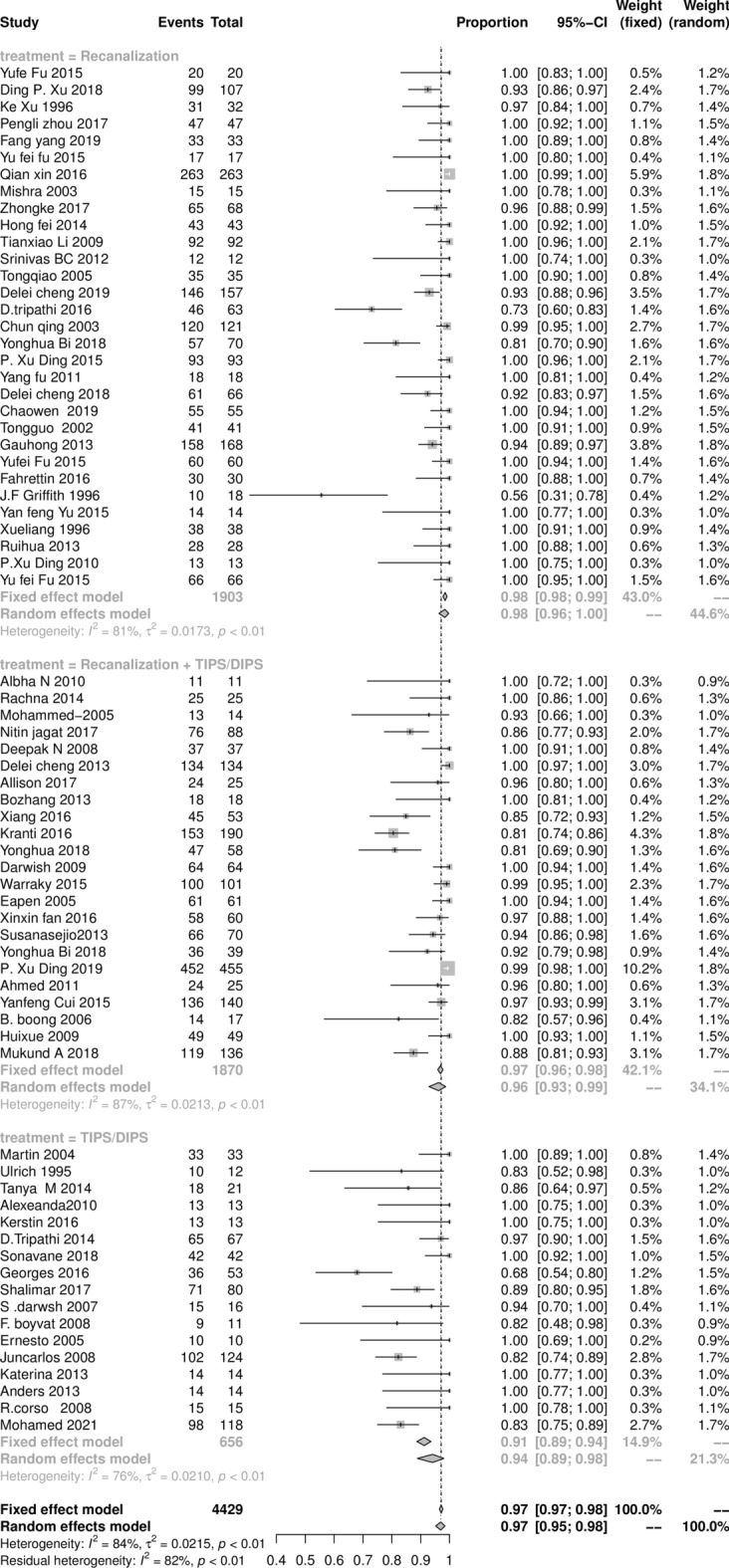
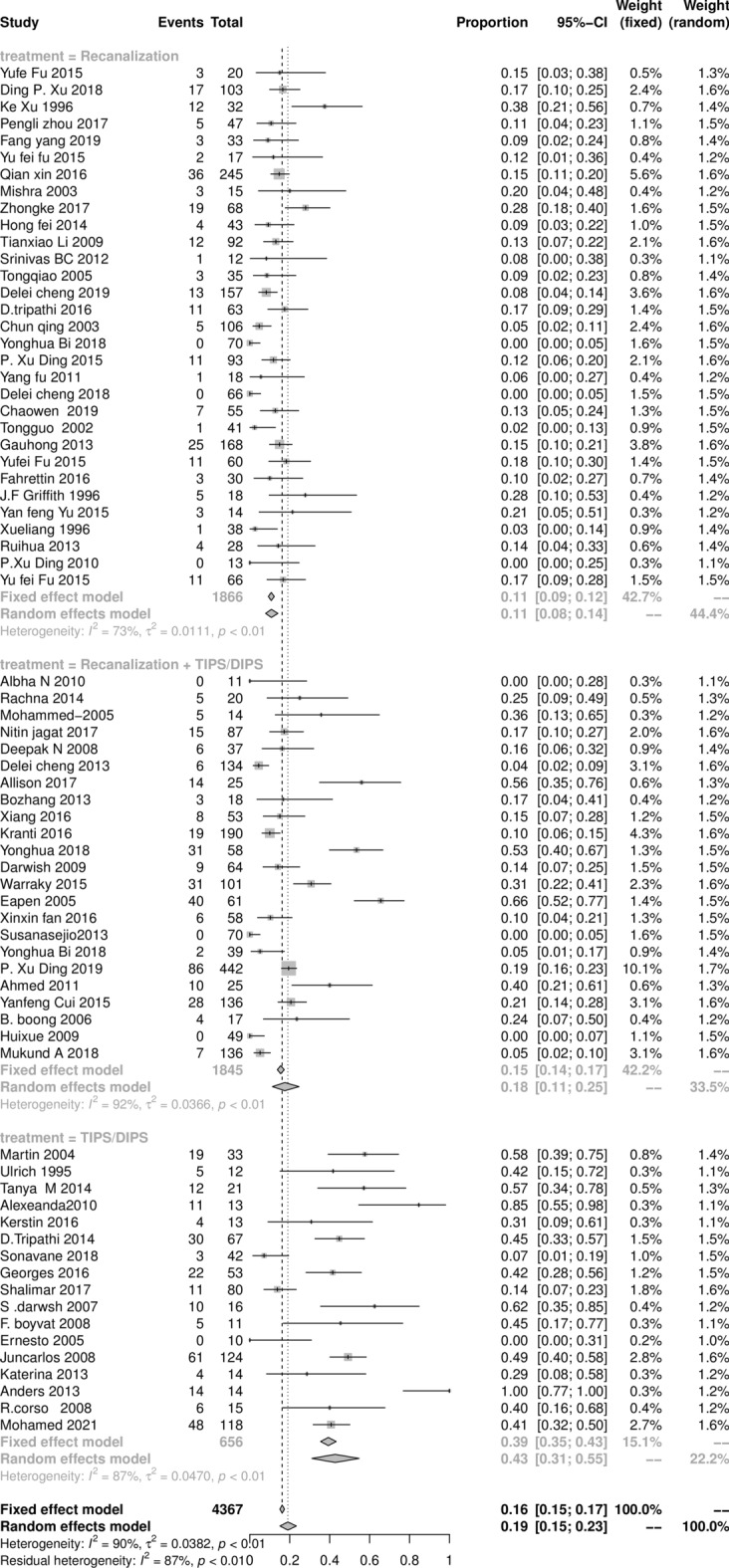
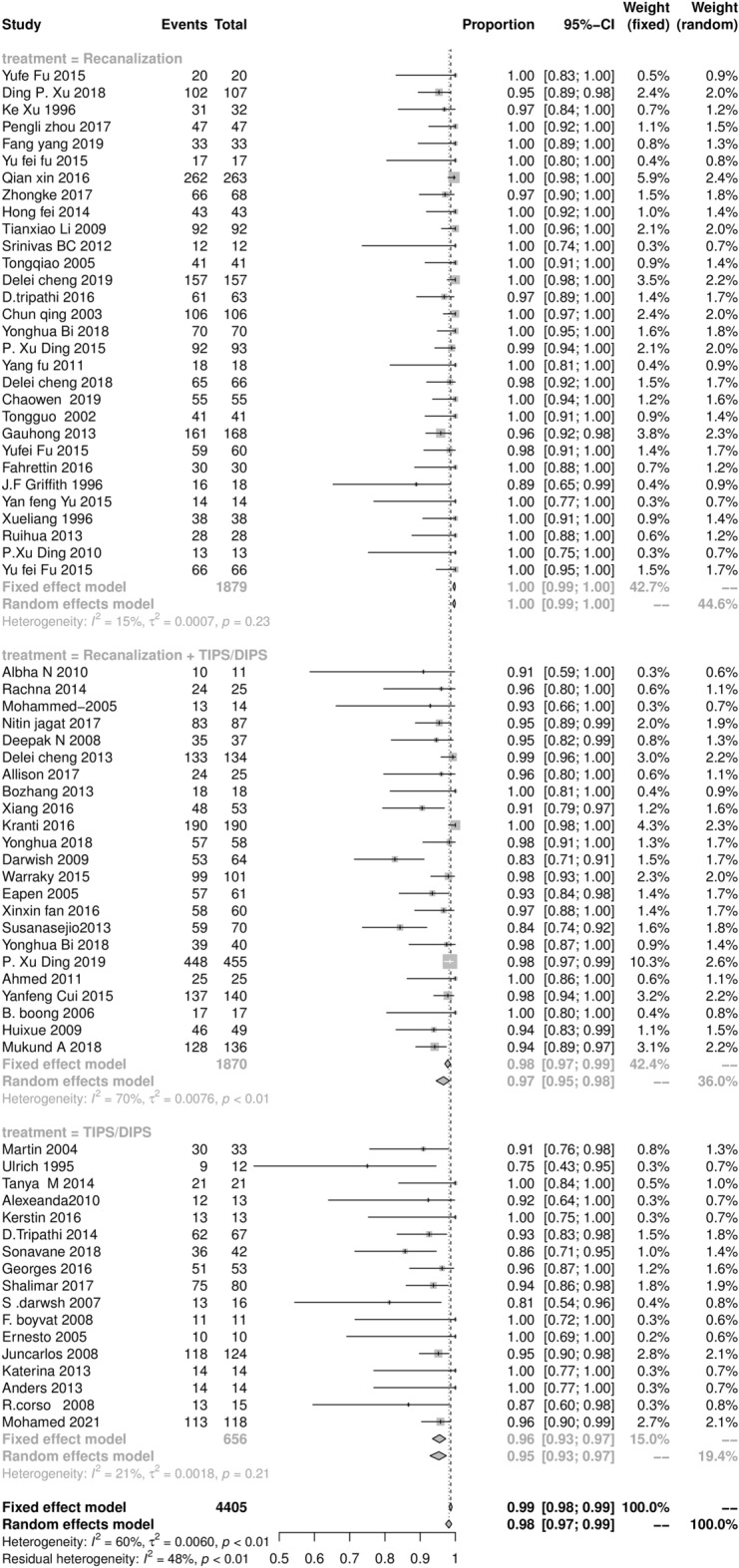
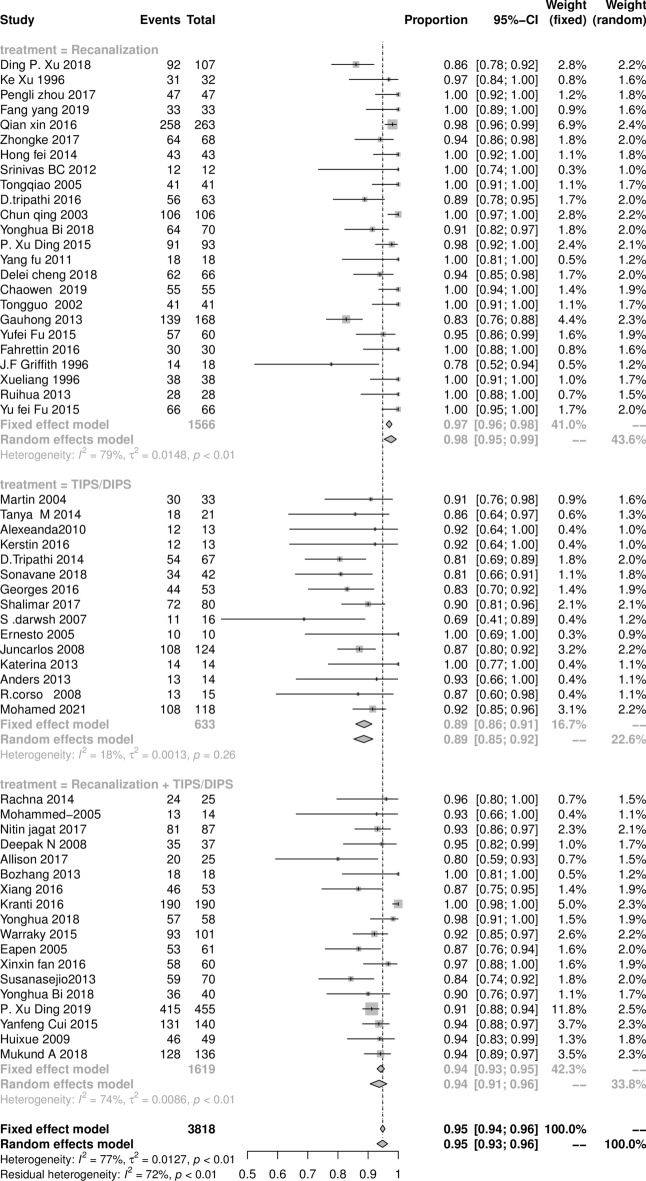
This study was performed to evaluate the outcome of endovascular intervention therapy for Budd-Chiari syndrome (BCS) and compare recanalization, transjugular intrahepatic portosystemic shunt (TIPS)/direct intrahepatic portosystemic shunt (DIPS), and combined procedure treatment. For the meta-analysis, 71 studies were identified by searching four databases. The individual studies' samples were used to calculate a confidence interval (CI 95%), and data were pooled using a fixed-effect model and random effect model. The pooled measure and an equal-weighted average rate were calculated in all participant studies. Heterogeneity between the studies was assessed with I2, and T2 tests, and publication bias was estimated using Egger's regression test. A total of 4,407 BCS patients had undergone an endovascular intervention procedure. The pooled results were 98.9% (95% CI 97.8‒98.9%) for a technical success operation, and 96.9% (95% CI 94.9‒98.9%) for a clinical success operation. The re-intervention rate after the initial intervention procedure was 18.9% (95% CI 14.7‒22.9%), and the survival rates at 1 and 5 years after the initial intervention procedure were 98.9% (95% CI 96.8‒98.9%) and 94.9% (95% CI 92.9‒96.9%), respectively. Patients receiving recanalization treatment (98%) had a better prognosis than those with a combined procedure (95.6%) and TIPS/DIPS treatment (94.5%). The systematic review and meta-analysis further solidify the role of endovascular intervention treatment in BCS as safe and effective. It maintains high technical and clinical success and long-term survival rates. The recanalization treatment had a better prognosis and outcome than the combined procedures and TIPS/DIPS treatment.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Endovascular treatment of symptomatic Budd-Chiari syndrome - in favour of early transjugular intrahepatic portosystemic shunt.Eur J Gastroenterol Hepatol. 2016 Jun;28(6):656-60. doi: 10.1097/MEG.0000000000000621. Eur J Gastroenterol Hepatol. 2016. PMID: 26958788
-
Long-term Outcome and Analysis of Dysfunction of Transjugular Intrahepatic Portosystemic Shunt Placement in Chronic Primary Budd-Chiari Syndrome.Radiology. 2017 Apr;283(1):280-292. doi: 10.1148/radiol.2016152641. Epub 2016 Oct 31. Radiology. 2017. PMID: 27797679
-
Survival and clinical success of endovascular intervention in patients with Budd-Chiari syndrome: A systematic review.J Clin Imaging Sci. 2023 Jan 24;13:5. doi: 10.25259/JCIS_130_2022. eCollection 2023. J Clin Imaging Sci. 2023. PMID: 36751561 Free PMC article. Review.
-
TEN-YEAR OUTCOMES OF TIPS FOR BUDD-CHIARI SYNDROME: SYSTEMATIC REVIEW AND META-ANALYSIS.Arq Gastroenterol. 2024 Jun 17;61:e23171. doi: 10.1590/S0004-2803.24612023-171. eCollection 2024. Arq Gastroenterol. 2024. PMID: 38896573
-
Transjugular intrahepatic portosystemic shunt for severe jaundice in patients with acute Budd-Chiari syndrome.World J Gastroenterol. 2015 Feb 28;21(8):2413-8. doi: 10.3748/wjg.v21.i8.2413. World J Gastroenterol. 2015. PMID: 25741149 Free PMC article.
Cited by
-
Budd Chiari Syndrome with Portal Vein Thrombosis Managed Successfully with Direct Intrahepatic Portosystemic Shunt: A Case Report and Review of the Literature.J Clin Exp Hepatol. 2023 Sep-Oct;13(5):917-920. doi: 10.1016/j.jceh.2023.06.005. Epub 2023 Jun 19. J Clin Exp Hepatol. 2023. PMID: 37693264 Free PMC article.
-
Budd-Chiari Syndrome Secondary to Myelofibrosis in a Patient With Polycythemia Vera: A 16-Year Disease Progression Case Highlighting JAK2 Mutation Pathogenesis.Cureus. 2025 Apr 20;17(4):e82629. doi: 10.7759/cureus.82629. eCollection 2025 Apr. Cureus. 2025. PMID: 40395270 Free PMC article.
-
Interventions in Budd-Chiari syndrome: an updated review.Abdom Radiol (NY). 2025 Mar;50(3):1307-1319. doi: 10.1007/s00261-024-04558-4. Epub 2024 Sep 26. Abdom Radiol (NY). 2025. PMID: 39325211 Review.
-
Budd-Chiari Syndrome Caused by Polycythemia Vera: A Case Report.Cureus. 2023 Sep 19;15(9):e45527. doi: 10.7759/cureus.45527. eCollection 2023 Sep. Cureus. 2023. PMID: 37868390 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
