

Burden of influenza hospitalization among high-risk groups in the United States
- PMID: 36171601
- PMCID: PMC9520810
- DOI: 10.1186/s12913-022-08586-y
Burden of influenza hospitalization among high-risk groups in the United States
Abstract
Background: Seasonal influenza poses a substantial clinical and economic burden in the United States and vulnerable populations, including the elderly and those with comorbidities, are at elevated risk for influenza-related medical complications.
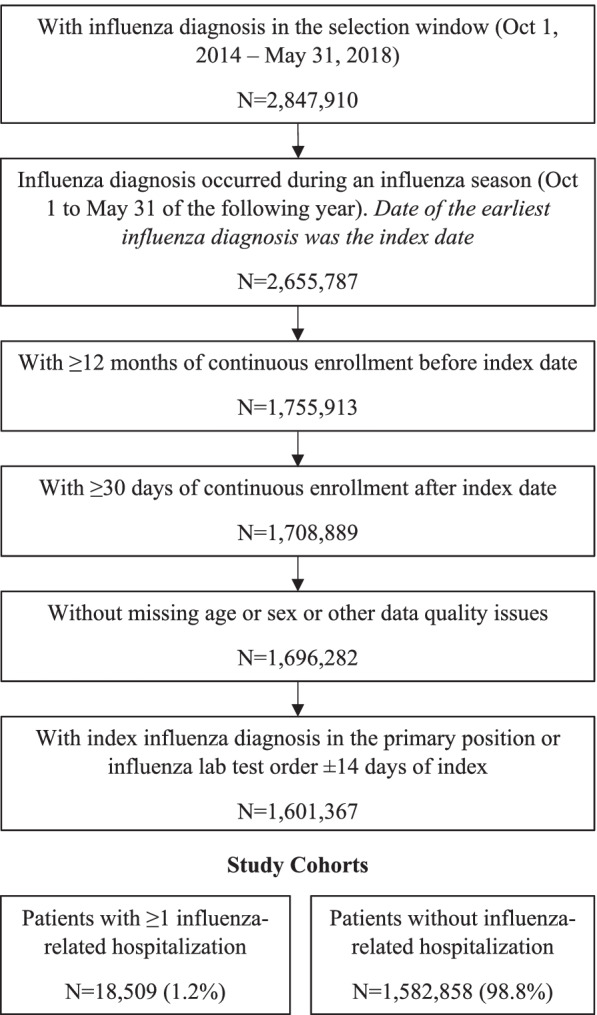
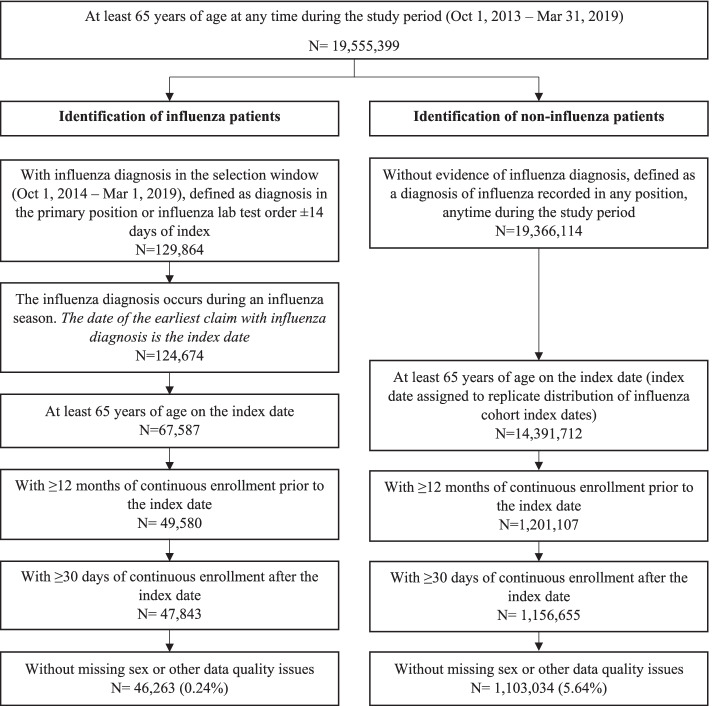
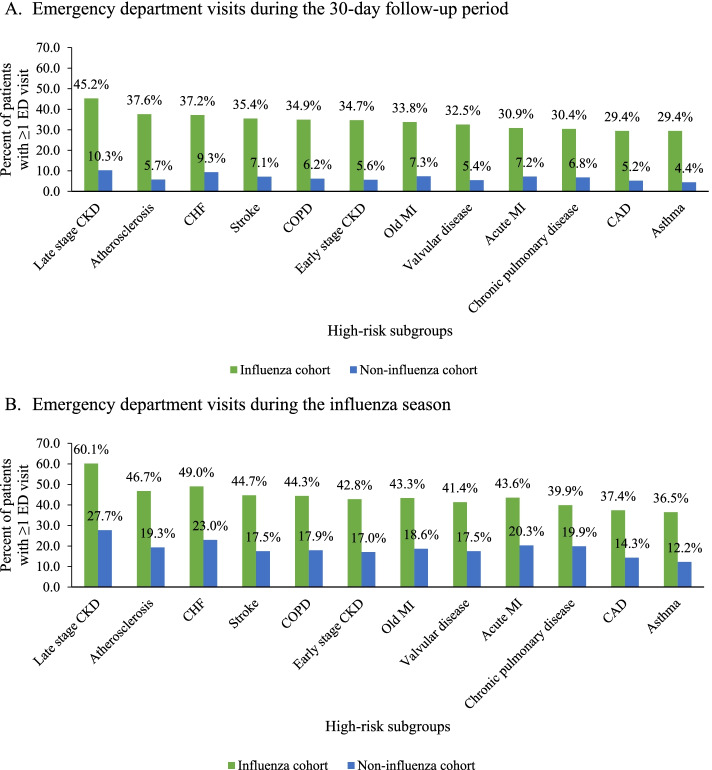
Methods: We conducted a retrospective cohort study using the IQVIA PharMetrics® Plus claims database in two stages. In Stage 1, we identified patients with evidence of medically-attended influenza during influenza seasons from October 1, 2014 to May 31, 2018 (latest available data for Stage 1) and used a multivariable logistic regression model to identify patient characteristics that predicted 30-day influenza-related hospitalization. The findings from Stage 1 informed high-risk subgroups of interest for Stage 2, where we selected cohorts of influenza patients during influenza seasons from October 1, 2014 to March 1, 2019 and used 1:1 propensity score matching to patients without influenza with similar high-risk characteristics to compare influenza-attributable rates of all-cause hospital and emergency department (ED) visits during follow-up (30-day and in the index influenza season).
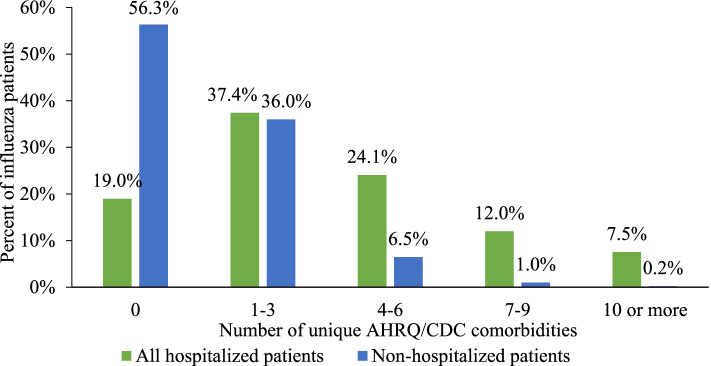
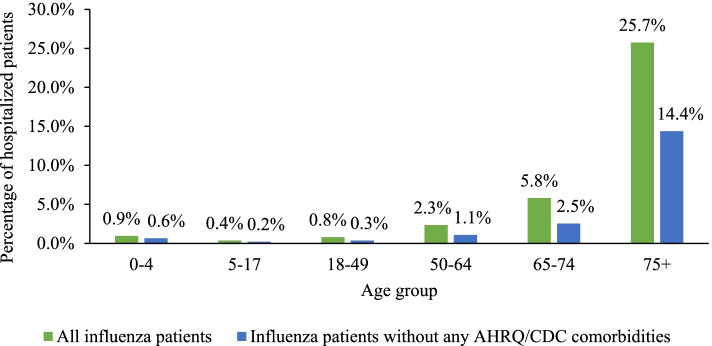
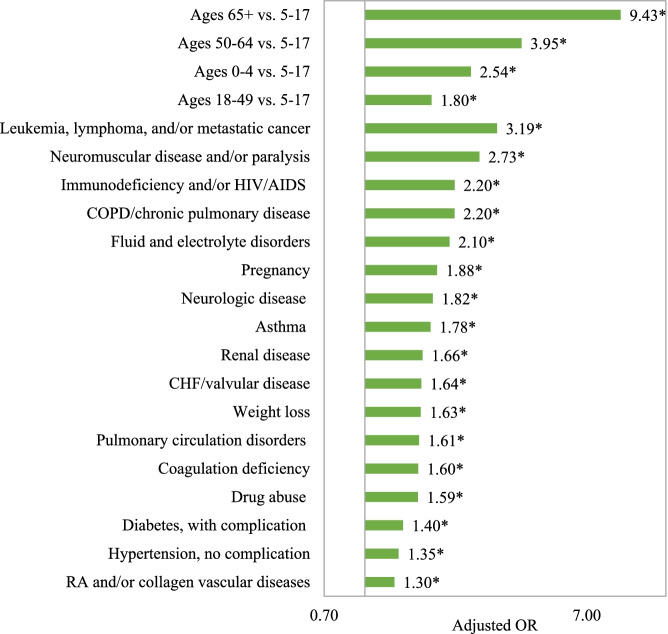
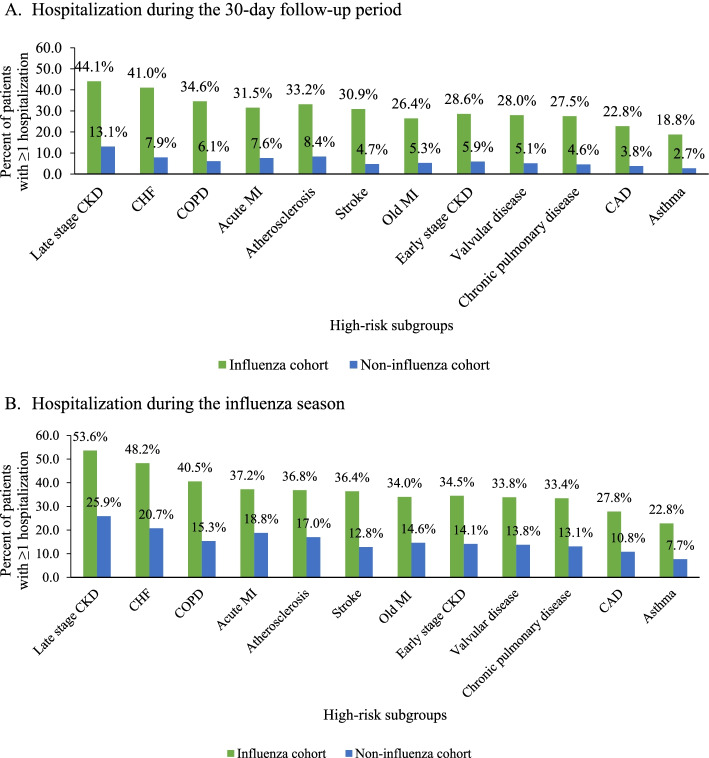
Results: In Stage 1, more than 1.6 million influenza cases were identified, of which 18,509 (1.2%) had a hospitalization. Elderly age was associated with 9 times the odds of hospitalization (≥65 years vs. 5-17 years; OR = 9.4, 95% CI 8.8-10.1) and select comorbidities were associated with 2-3 times the odds of hospitalization. In Stage 2, elderly influenza patients with comorbidities had 3 to 7 times higher 30-day hospitalization rates compared to matched patients without influenza, including patients with congestive heart failure (41.0% vs.7.9%), chronic obstructive pulmonary disease (34.6% vs. 6.1%), coronary artery disease (22.8% vs. 3.8%), and late-stage chronic kidney disease (44.1% vs. 13.1%; all p < 0.05).
Conclusions: The risk of influenza-related complications is elevated in the elderly, especially those with certain underlying comorbidities, leading to excess healthcare resource utilization. Continued efforts, beyond currently available vaccines, are needed to reduce influenza burden in high-risk populations.
Keywords: Comorbidities; Health resource utilization; Hospitalization; Influenza; Real-world.
© 2022. The Author(s).
Conflict of interest statement
D.H. and C.R. reports financial support from VIR Biotechnology Inc. Y.Y. reports a relationship with VIR Biotechnology Inc. that includes: funding grants. D.H. reports a relationship with Janssen Pharmaceuticals Inc. that includes: employment. D.H. reports a relationship with VIR Biotechnology Inc. that includes: equity or stocks. C.R. reports a relationship with VIR Biotechnology Inc. that includes: employment and equity or stocks. A.N. and J.T. are employees of IQVIA, which received funding from VIR Biotechnology Inc. to conduct this study.
Figures
References
-
- Centers for Disease Control and Prevention . Disease Burden of Influenza. 2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
