

Evaluation of analgesic effects and hemodynamic responses of epidural ropivacaine in laparoscopic abdominal surgeries: Randomised controlled trial
- PMID: 36171946
- PMCID: PMC9511868
- DOI: 10.4103/joacp.JOACP_153_20
Evaluation of analgesic effects and hemodynamic responses of epidural ropivacaine in laparoscopic abdominal surgeries: Randomised controlled trial
Abstract
Background and aims: The role of epidural analgesia in laparoscopic surgeries remains controversial. We evaluated intraoperative analgesic effects of epidural ropivacaine versus intravenous fentanyl in laparoscopic abdominal surgery and assessed postoperative analgesic requirements, hemodynamic changes, time to ambulation, and length of stay (LOS) in the ICU.
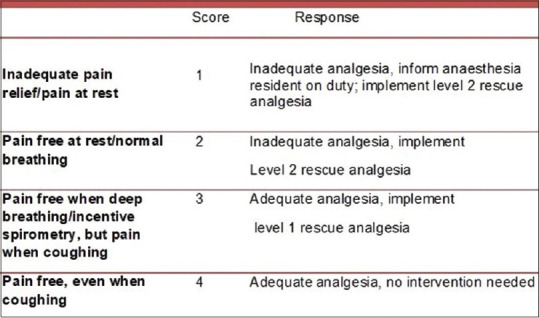
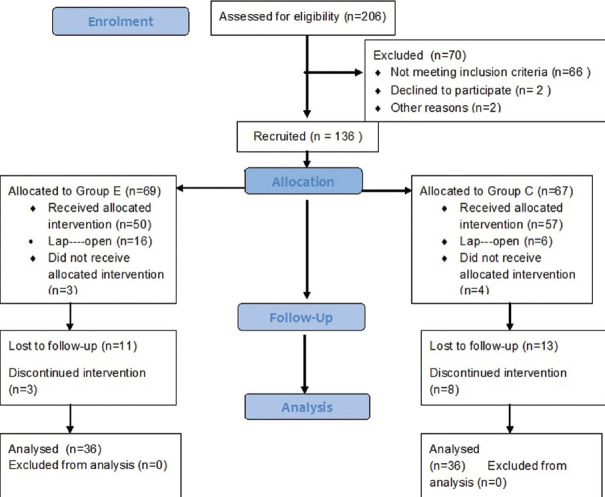
Material and methods: Seventy-two American Society of Anesthesiologists physical status I-III adult patients undergoing elective laparoscopic abdominal surgeries were randomized to either 0.5 mg/kg/h intravenous fentanyl (Group C) or 0.2% epidural ropivacaine at 5-8 mL/h (Group E) infusions intraoperatively and 0.25 m/kg/h fentanyl and 0.1% epidural ropivacaine infusions respectively postoperatively. Variations in mean arterial pressure (MAP) of 20% from baseline were points of intervention for propofol and analgesia with fentanyl or vasopressors. The number of interventions and total doses of fentanyl and vasopressors were noted. Postoperative analgesia was assessed at 0, 6, 12, and 24 h and when pain was reported with numerical rating scale and objective pain scores. Chi-square test and Student's t-test were used for categorical and continuous variable analysis.
Results: Intraoperatively, 14 patients versus 4 needed additional fentanyl and 26 versus 14 needed additional propofol in groups C and E respectively (P = 0.007, P = 0.004). MAP at 0, 6 and 18 h was lower in Group E. Pain scores were better in Group E at 6,18, and 24 h postoperatively. Time to ambulation was comparable but LOS ICU was prolonged in Group E (P = 0.05).
Conclusion: Epidural ropivacaine produces superior intraoperative analgesia and improved postoperative pain scores without affecting ambulation but increases vasopressor need and LOS ICU in comparison with intravenous fentanyl in laparoscopic abdominal surgeries.
Keywords: Epidural analgesia; laparoscopy; ropivacaine.
Copyright: © 2022 Journal of Anaesthesiology Clinical Pharmacology.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Intravenous Lignocaine-Fentanyl Versus Epidural Ropivacaine-Fentanyl for Postoperative Analgesia After Major Abdominal Oncosurgery: A Pilot Prospective Randomised Study.Turk J Anaesthesiol Reanim. 2021 Apr;49(2):130-137. doi: 10.5152/TJAR.2020.23326. Epub 2020 Feb 17. Turk J Anaesthesiol Reanim. 2021. PMID: 33997842 Free PMC article.
-
Comparison of ropivacaine with and without fentanyl vs bupivacaine with fentanyl for postoperative epidural analgesia in bilateral total knee replacement surgery.J Clin Anesth. 2017 Feb;37:7-13. doi: 10.1016/j.jclinane.2016.08.020. Epub 2016 Dec 22. J Clin Anesth. 2017. PMID: 28235533 Clinical Trial.
-
Comparative Evaluation of Ropivacaine and Fentanyl Versus Ropivacaine and Fentanyl with Clonidine for Postoperative Epidural Analgesia in Total Knee Replacement Surgery.J Clin Diagn Res. 2017 Sep;11(9):UC09-UC12. doi: 10.7860/JCDR/2017/25401.10615. Epub 2017 Sep 1. J Clin Diagn Res. 2017. PMID: 29207811 Free PMC article.
-
Comparative Analysis of the Postoperative Analgesic Effects of Caudal Epidural Injection of Ropivacaine Combined With Fentanyl Versus Ropivacaine Alone in Lumbosacral Spine Surgeries: A Randomized Double-Blinded Study.Cureus. 2024 Oct 6;16(10):e70963. doi: 10.7759/cureus.70963. eCollection 2024 Oct. Cureus. 2024. PMID: 39507136 Free PMC article.
-
Comparison of continuous epidural infusion of 0.125% ropivacaine with 1 μg/ml fentanyl versus 0.125% bupivacaine with 1 μg/ml fentanyl for postoperative analgesia in major abdominal surgery.J Anaesthesiol Clin Pharmacol. 2018 Jan-Mar;34(1):29-34. doi: 10.4103/joacp.JOACP_122_16. J Anaesthesiol Clin Pharmacol. 2018. PMID: 29643619 Free PMC article.
Cited by
-
Anesthetics as an Alternative to Opioids in Laparoscopic Surgeries: An Observational Study.Cureus. 2025 Jun 20;17(6):e86421. doi: 10.7759/cureus.86421. eCollection 2025 Jun. Cureus. 2025. PMID: 40689002 Free PMC article.
-
Role of an epidural in laparoscopic surgeries.J Anaesthesiol Clin Pharmacol. 2024 Apr-Jun;40(2):365. doi: 10.4103/joacp.joacp_329_22. Epub 2023 Apr 7. J Anaesthesiol Clin Pharmacol. 2024. PMID: 38919436 Free PMC article. No abstract available.
References
-
- Bruce J, Krukowski ZH. Quality of life and chronic pain four years after gastrointestinal surgery. Dis Colon Rectum. 2006;49:1362–70. - PubMed
-
- Wind J, Polle SW, Fung Kon Jin PH, Dejong CH, von Meyenfeldt MF, Ubbink DT, et al. Laparoscopy and/or Fast Track Multimodal Management Versus Standard Care (LAFA) Study Group;Enhanced Recovery after Surgery (ERAS) Group. Systematic review of enhanced recovery programmes in colonic surgery. Br J Surg. 2006;93:800–9. - PubMed
-
- Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery. Enhanced Recovery After Surgery (ERAS) Recommendations:|y2018. World J Surg. 2019;43:659–95. - PubMed
LinkOut - more resources
Full Text Sources