

Characteristics of myeloproliferative neoplasm-associated portal hypertension and endoscopic management of variceal bleeding
- PMID: 36172080
- PMCID: PMC9511301
- DOI: 10.1177/20406223221125691
Characteristics of myeloproliferative neoplasm-associated portal hypertension and endoscopic management of variceal bleeding
Abstract
Background: Myeloproliferative neoplasms (MPNs) are a rare yet important clinical cause of portal hypertension, which may cause recurrent gastroesophageal variceal bleeding (GVB). MPN-associated variceal bleeding lacks specific guidelines and clinical consensus and desiderates cohort studies. We performed a multicenter retrospective study to investigate the efficacy of endoscopic management of bleeding in MPNs.
Methods: We included consecutive MPN patients with gastroesophageal varices in eight tertiary university hospitals between January 2007 and March 2020. The clinical characteristics of participants were summarized. MPN patients with a history of GVB were followed up for the rebleeding and death, compared with controls suffering from schistosomiasis-associated portal hypertension who received endoscopic treatment for variceal bleeding at the same period.
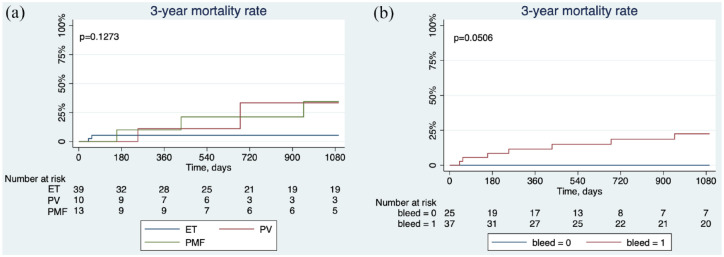
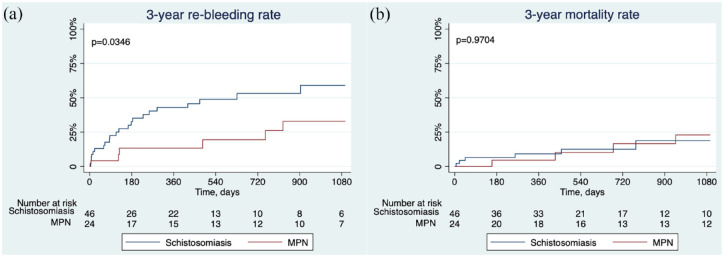
Results: A total of 62 MPN patients with gastroesophageal varices were identified, and 37 had a history of GVB. Of these, 24 patients received endoscopic variceal ligation and endoscopic injection of cyanoacrylate for the prophylaxis of variceal rebleeding. Endoscopic treatment significantly reduced the rebleeding rate in MPN patients with a history of GVB (28.2% versus 68.3%, p = 0.0269). Multivariable Cox regression indicated that endoscopic treatment (HR = 0.10, 95% CI: 0.02-0.54, p = 0.008) was the independent protective factor for decreasing the 3-year rebleeding rate, while the use of non-selective beta-blockers (NSBB) (HR = 13.41, 95% CI: 2.15-83.42, p = 0.005) was the risk factor for increasing the 3-year rebleeding rate. As for the efficacy of endoscopic management, 3-year rebleeding rate was significantly lower in MPN patients in contrast to 46 controls with schistosomiasis-associated variceal bleeding (32.9% versus 59.0%, p = 0.0346).
Conclusion: Endoscopic treatment might be a feasible and potent approach in the management of gastroesophageal variceal rebleeding in MPNs, while NSBB might be ineffective.
Keywords: Janus kinase 2; chronic hematologic malignancy; endoscopy; gastroesophageal varices; non-cirrhotic portal hypertension; rebleeding prophylaxis.
© The Author(s), 2022.
Conflict of interest statement
Competing interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The article has been read and approved by all the authors.
Figures



Similar articles
-
Endoscopic treatment of gastroesophageal variceal bleeding after oxaliplatin-based chemotherapy in patients with colorectal cancer.Endoscopy. 2020 Sep;52(9):727-735. doi: 10.1055/a-1157-8611. Epub 2020 May 7. Endoscopy. 2020. PMID: 32380558
-
Partial splenic embolization combined with endoscopic therapies and NSBB decreases the variceal rebleeding rate in cirrhosis patients with hypersplenism: a multicenter randomized controlled trial.Hepatol Int. 2021 Jun;15(3):741-752. doi: 10.1007/s12072-021-10155-0. Epub 2021 Feb 27. Hepatol Int. 2021. PMID: 33638769 Free PMC article. Clinical Trial.
-
Aluminum phosphate gel reduces early rebleeding in cirrhotic patients with gastric variceal bleeding treated with histoacryl injection therapy.World J Gastrointest Endosc. 2023 Mar 16;15(3):153-162. doi: 10.4253/wjge.v15.i3.153. World J Gastrointest Endosc. 2023. PMID: 37034972 Free PMC article.
-
[Endoscopic Treatment and Prevention of Acute Variceal Hemorrhage].Korean J Helicobacter Up Gastrointest Res. 2024 Mar;24(1):5-15. doi: 10.7704/kjhugr.2024.0005. Epub 2024 Mar 8. Korean J Helicobacter Up Gastrointest Res. 2024. PMID: 40503288 Free PMC article. Review. Korean.
-
Variceal and other portal hypertension related bleeding.Best Pract Res Clin Gastroenterol. 2013 Oct;27(5):649-64. doi: 10.1016/j.bpg.2013.08.004. Epub 2013 Sep 5. Best Pract Res Clin Gastroenterol. 2013. PMID: 24160925 Review.
References
-
- Khanna R, Sarin SK. Non–cirrhotic portal hypertension – diagnosis and management. J Hepatol 2014; 60: 421–441. - PubMed
-
- Arber DA, Orazi A, Hasserjian R, et al.. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016; 127: 2391–2405. - PubMed
-
- Zhao G, Wu ZY, Zhang B, et al.. Diagnosis and treatment of portal hypertension secondary to myeloproliferative disorders: a report of three cases. J Dig Dis 2011; 12: 312–316. - PubMed
-
- Kander EM, Raza S, Zhou Z, et al.. Bleeding complications in BCR-ABL negative myeloproliferative neoplasms: prevalence, type, and risk factors in a single-center cohort. Int J Hematol 2015; 102: 587–593. - PubMed
-
- Foucar CE, Stein BL. JAK2 V617F mutation testing in patients presenting with hepatic and portal vein thrombosis. JAMA 2017; 317: 2228–2229. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
