

Associations between dietary fiber intake and cardiovascular risk factors: An umbrella review of meta-analyses of randomized controlled trials
- PMID: 36172520
- PMCID: PMC9511151
- DOI: 10.3389/fnut.2022.972399
Associations between dietary fiber intake and cardiovascular risk factors: An umbrella review of meta-analyses of randomized controlled trials
Abstract
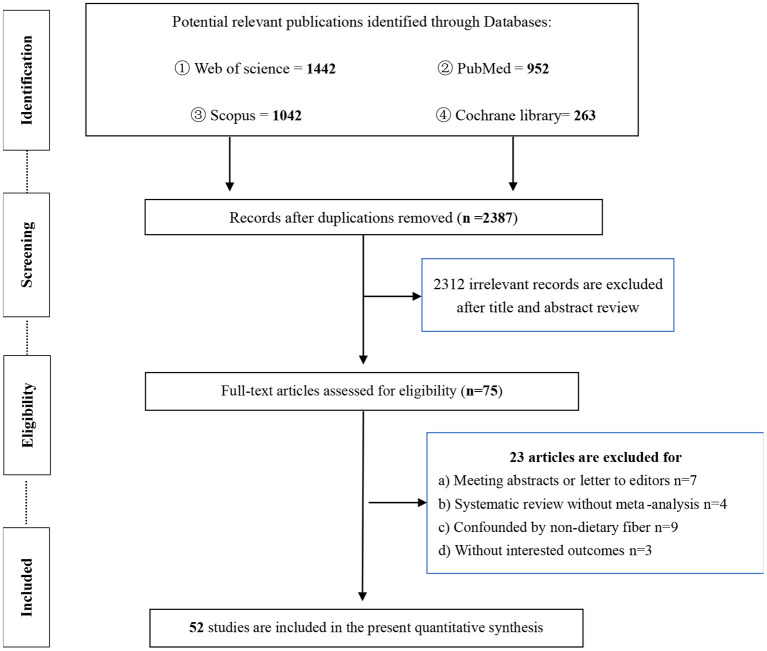
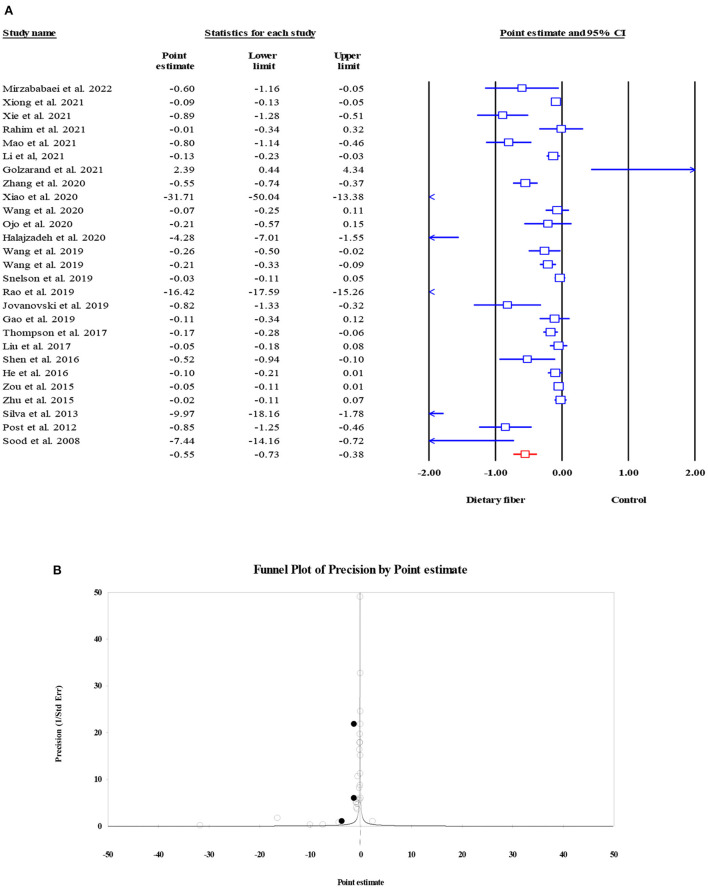
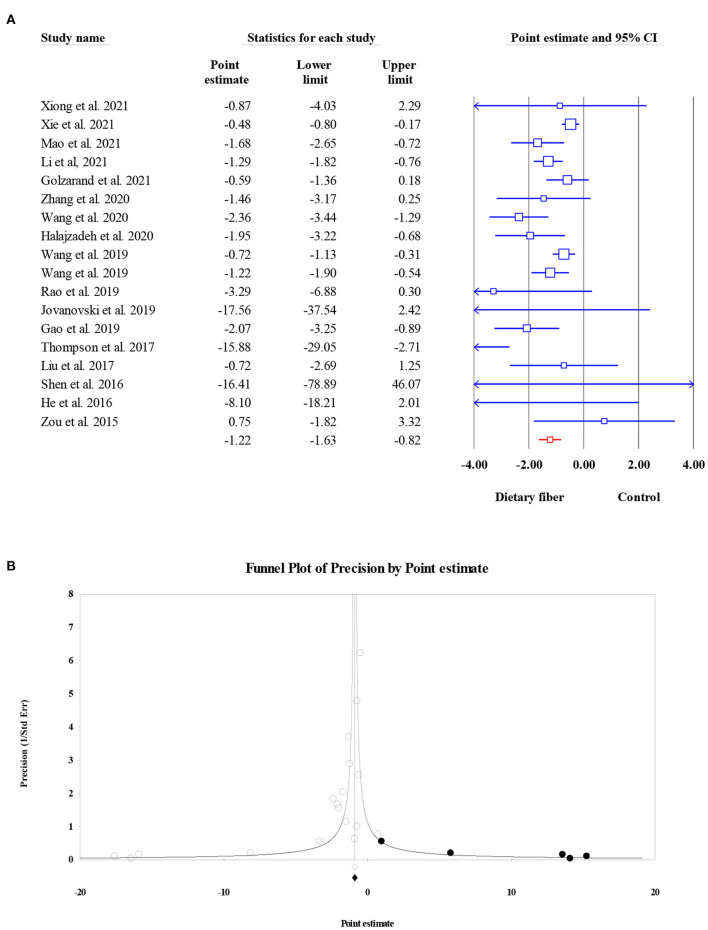
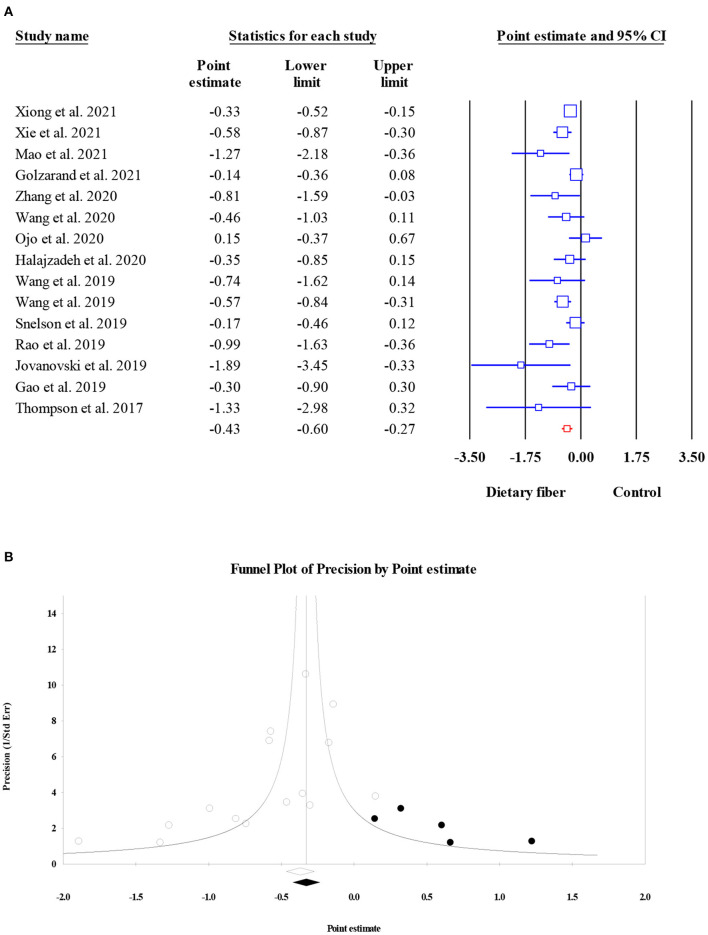
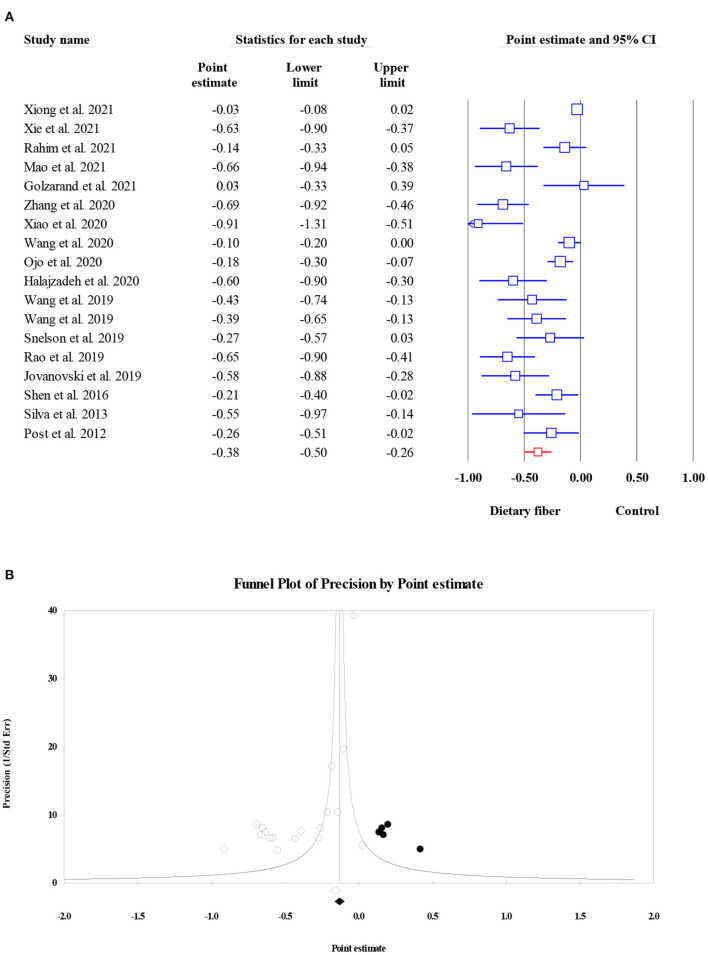
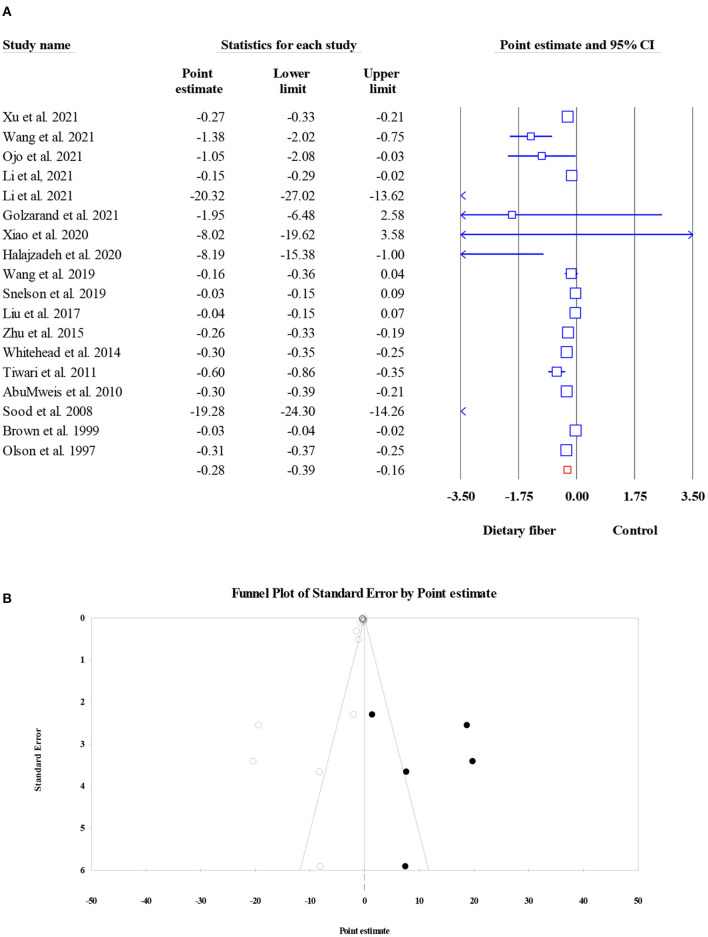
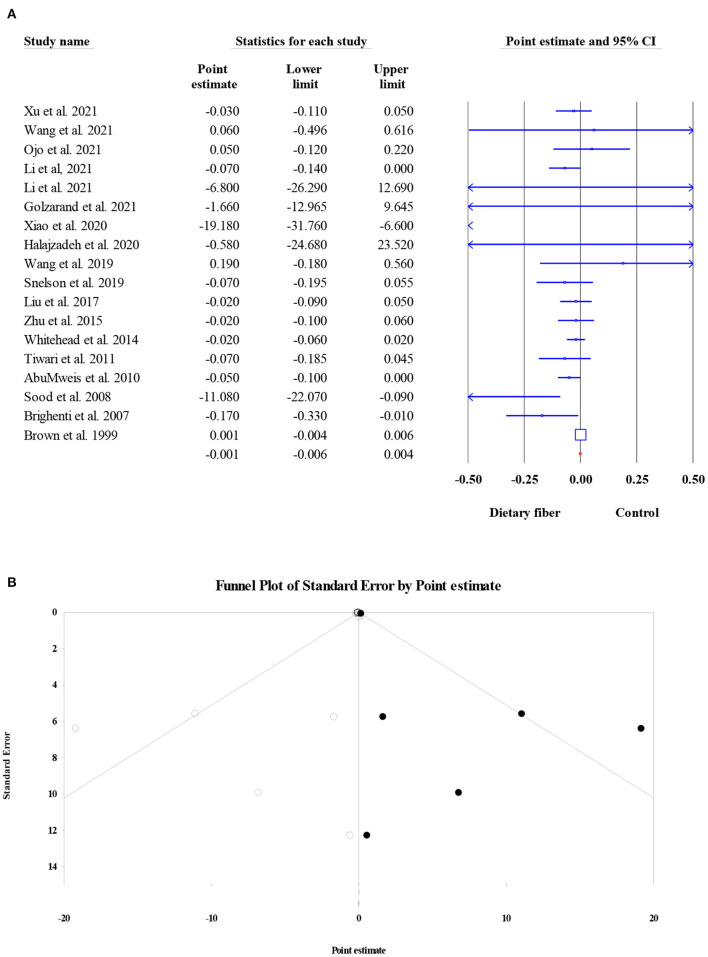
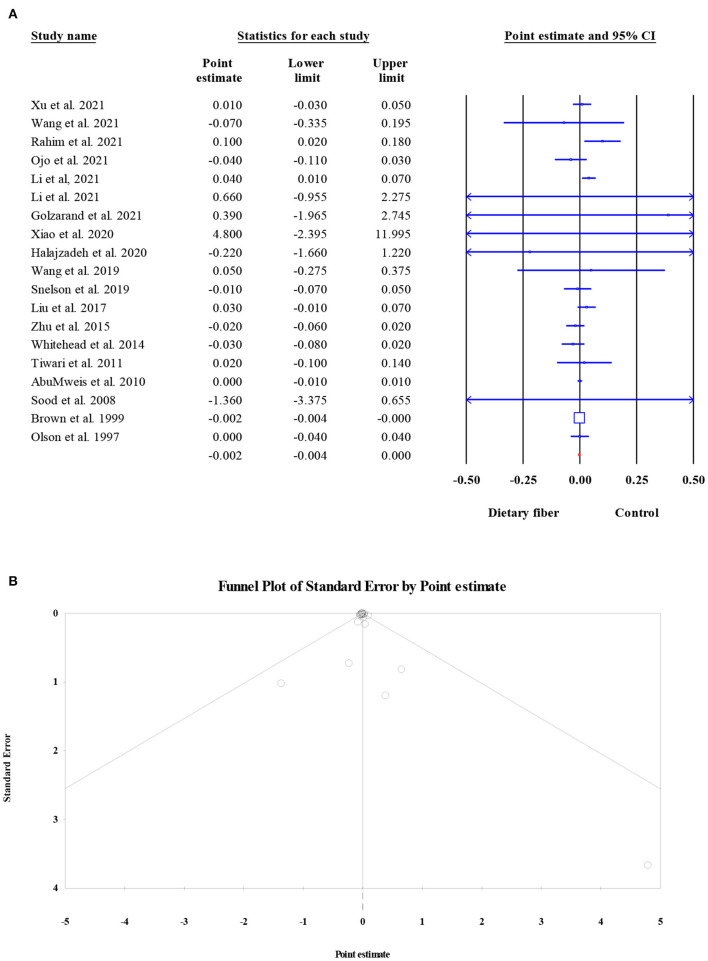
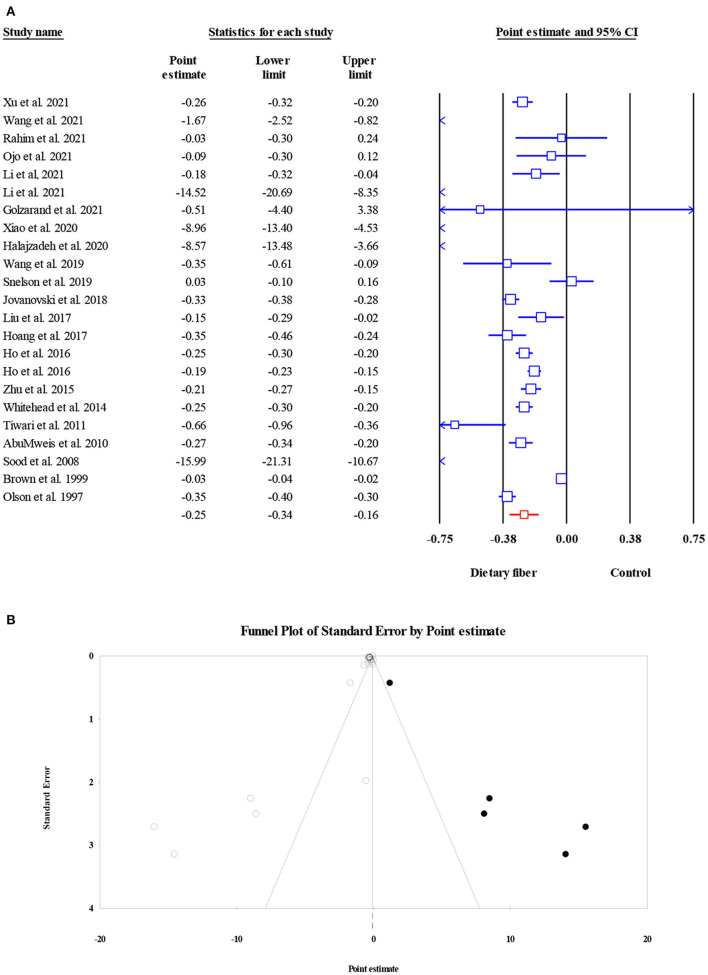
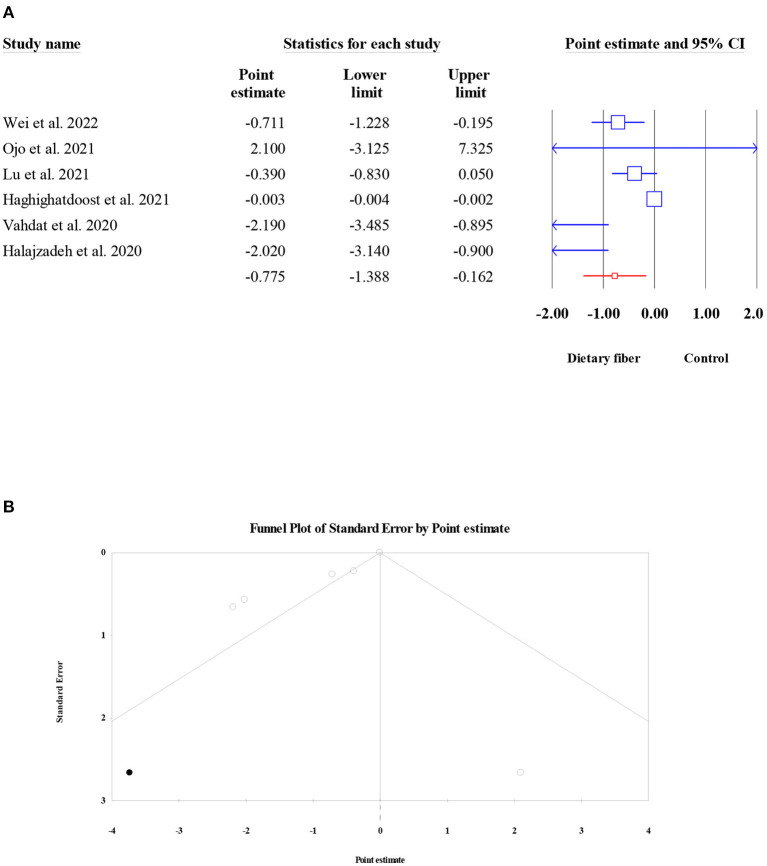
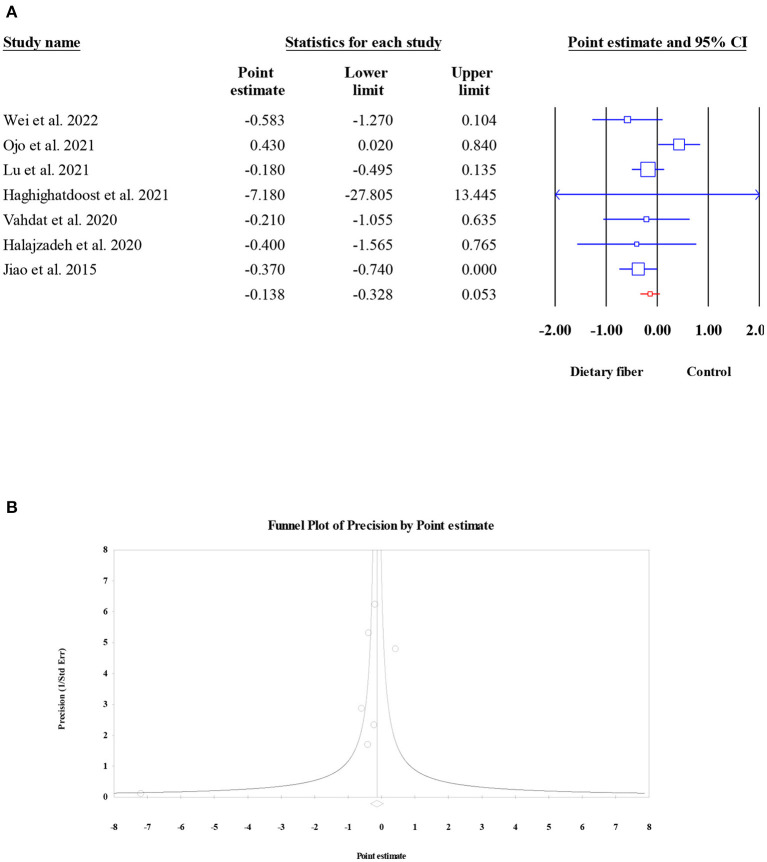
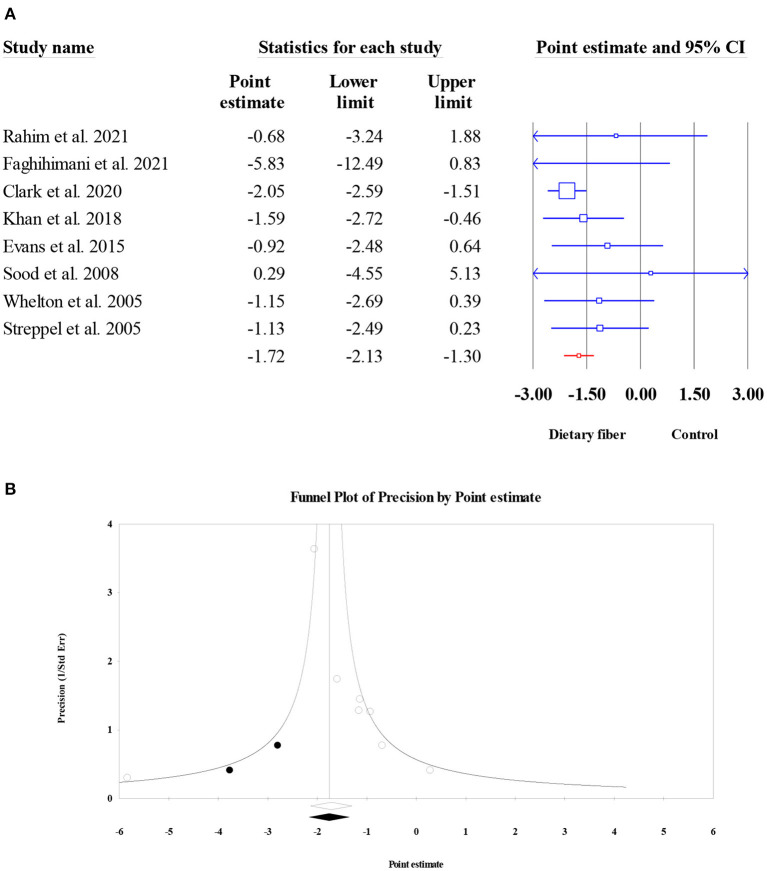
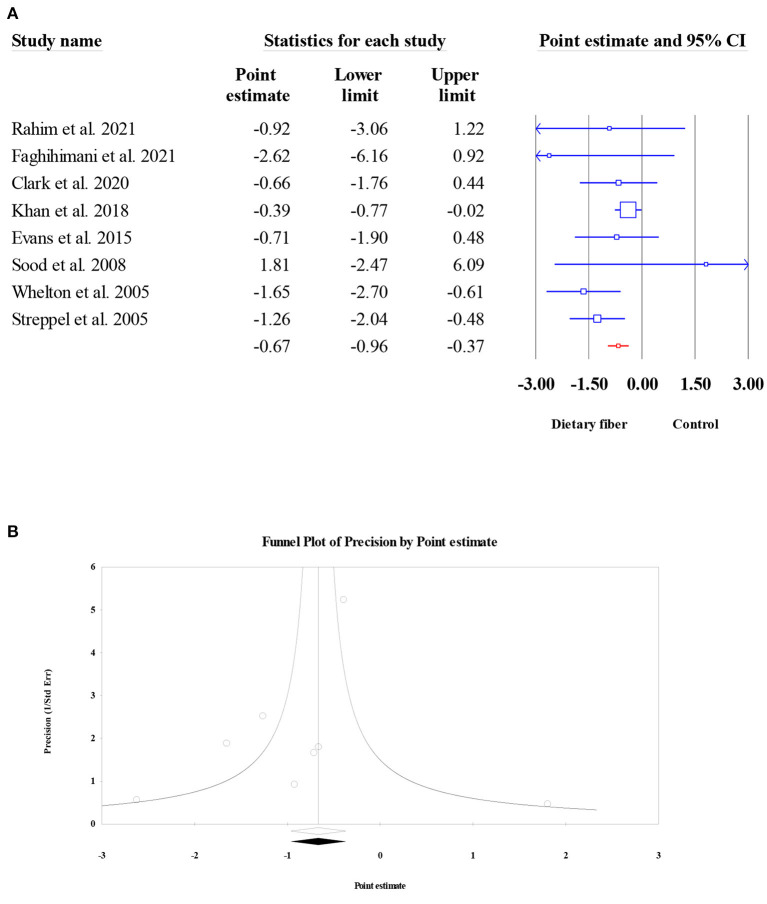
Although several meta-analyses have revealed the beneficial effects of dietary fiber intake on human health, some have reported inconsistent findings. The purpose of this work was to perform an umbrella meta-analysis to evaluate the relevant evidence and elucidate the effect of dietary fiber intake on glycemic control, lipid profiles, systematic inflammation, and blood pressure. Eligible studies were searched in several electronic databases, including Web of Science, PubMed, Scopus, and the Cochrane Library, up to March 2022. A total of 52 meta-analyses involving 47,197 subjects were identified to assess the pooled effect size. Overall, higher dietary fiber intake was significantly associated with reductions in parameters involving glycemic control, including fasting plasma glucose (ES = -0.55, 95% CI: -0.73, -0.38, P < 0.001), fasting plasma insulin (ES = -1.22, 95% CI: -1.63, -0.82, P < 0.001), homeostasis model assessment of insulin resistance (HOMA-IR) (ES = -0.43, 95% CI: -0.60, -0.27, P < 0.001), and glycosylated hemoglobin (HbA1c) (ES = -0.38, 95% CI: -0.50, -0.26, P < 0.001). In terms of lipid profiles, higher dietary fiber intake was associated with significant reductions in the serum level of total cholesterol (ES = -0.28, 95% CI: -0.39, -0.16, P < 0.001) and low-density lipoprotein cholesterol (ES = -0.25, 95% CI: -0.34, -0.16, P < 0.001), but not triglycerides (ES = -0.001, 95% CI: -0.006, 0.004, P = 0.759) and high-density lipoprotein cholesterol (ES = -0.002, 95% CI: -0.004, 0.000, P = 0.087). Higher dietary fiber intake was also significantly associated with improved tumor necrosis factor-alpha serum levels (ES = -0.78, 95% CI: -1.39, -0.16, P = 0.013), while no significant effect was observed for C-reactive protein (ES = -0.14, 95% CI: -0.33, 0.05, P = 0.156). Finally, blood pressure was also significantly improved following higher dietary fiber intake (systolic blood pressure: ES = -1.72, 95% CI: -2.13, -1.30, P < 0.001; diastolic blood pressure: ES = -0.67, 95% CI: -0.96, -0.37, P < 0.001). Subgroup analysis revealed that the study population and type of dietary fiber could be partial sources of heterogeneity. In conclusion, the present umbrella meta-analysis provides evidence for the role of dietary fiber supplementation in the improvement of established cardiovascular risk factors.
Keywords: blood pressure; dietary fiber; glycolipid metabolism; inflammation; umbrella meta-analysis.
Copyright © 2022 Fu, Zhang, Qian, Zhang and Tan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- World Health Organization. Health Topics of Cardiovascular Diseases. (2021). Available online at: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1
-
- Stanaway JD, Afshin A, Gakidou E, Lim SS, Abate D, Abate KH, et al. . Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1923–94. 10.1016/S0140-6736(18)32225-6 - DOI - PMC - PubMed
-
- China TW. CotRoCHaDi. Report on Cardiovascular Health and Diseases Burden in China: an Updated Summary of 2020 (2021).
Publication types
LinkOut - more resources
Full Text Sources
Research Materials