

Cranial thoracic myelopathies (T1-T6 vertebrae): Retrospective evaluation of the signalment, clinical presentation, and, presumptive or final diagnoses in 84 dogs
- PMID: 36172605
- PMCID: PMC9510707
- DOI: 10.3389/fvets.2022.960912
Cranial thoracic myelopathies (T1-T6 vertebrae): Retrospective evaluation of the signalment, clinical presentation, and, presumptive or final diagnoses in 84 dogs
Abstract
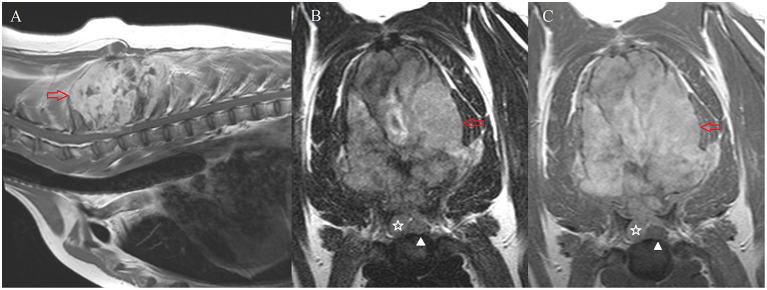
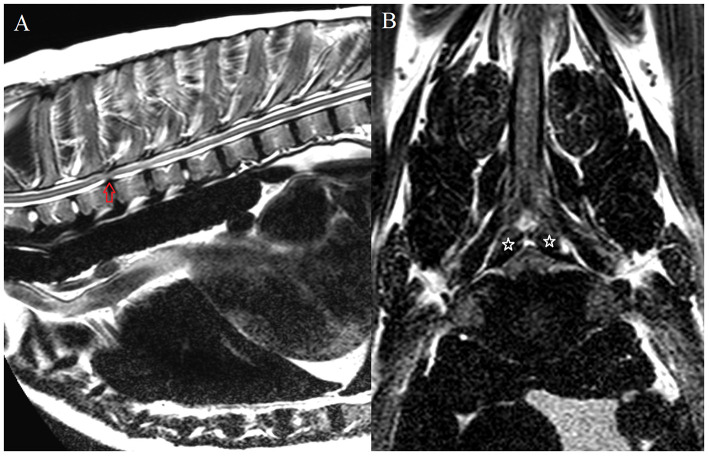
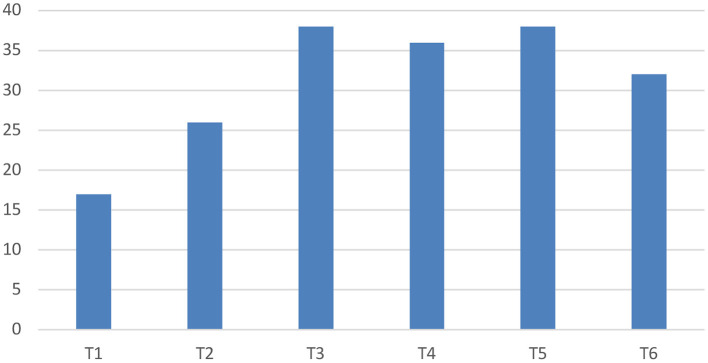
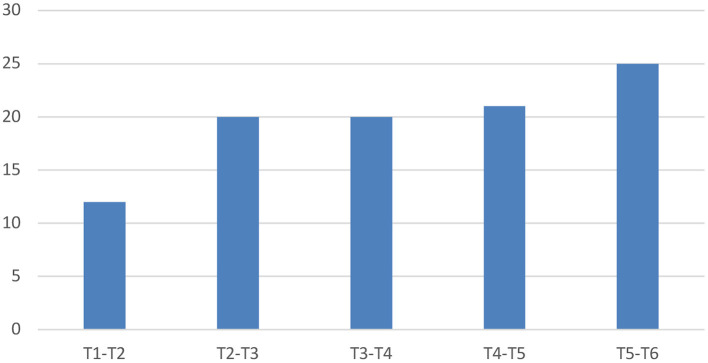
The aim of the study was to describe the signalment, clinical presentation and presumptive or final diagnoses of dogs with cranial thoracic spinal cord lesions identified on advanced imaging. Retrospective evaluation of the databases of three veterinary specialty centres, between 2009 and 2021, was performed to identify dogs with a lesion affecting the cranial thoracic vertebral column (T1-T6 vertebrae) as the primary cause for presenting signs of myelopathy and/or spinal pain. Eighty-four dogs were included in the study, with the majority (n = 76) presenting with a progressive history of over 4-weeks' duration. On neurologic examination, most dogs were ambulatory (n = 64), and the most common neuroanatomic localisation was the T3-L3 spinal cord segments (n = 63). Twelve dogs (14%) showed a short-strided thoracic limb gait on clinical examination. The most common diagnosis was neoplasia (n = 33), followed by anomalies (n = 22, including vertebral body malformations in 14 dogs) and degenerative disorders (n = 16, with intervertebral disc protrusion diagnosed in 9 dogs). The most common vertebrae affected were T3 and T5. Most dogs with degenerative conditions showed asymmetric clinical signs, and the majority of dogs with neoplasia showed signs of spinal hyperaesthesia on examination. The findings of this study describe the clinical signs and presumptive or final diagnoses associated with lesions affecting the cranial thoracic spinal cord. When combined with the signalment and clinical history, this information can assist in both the recognition of and problem-based approach to these cases.
Keywords: advanced imaging; ataxia; canine; neoplasia; neurological; spinal cord; two-engine gait.
Copyright © 2022 Lopes, Ives, José-López, Gutierrez-Quintana, Abouzeid, Freeman, Redondo and Sánchez-Masián.
Conflict of interest statement
Authors BL, EI, and DS-M were employed by Linnaeus Veterinary Limited. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Demographics, clinical findings and diagnoses of cranial thoracic myelopathies (T1-T6 vertebrae) in cats.J Feline Med Surg. 2023 Oct;25(10):1098612X231199731. doi: 10.1177/1098612X231199731. J Feline Med Surg. 2023. PMID: 37791892 Free PMC article.
-
Clinical reasoning in canine spinal disease: what combination of clinical information is useful?Vet Rec. 2015 Aug 15;177(7):171. doi: 10.1136/vr.102988. Epub 2015 Jul 21. Vet Rec. 2015. PMID: 26198211
-
Prevalence, clinical presentation, and etiology of myelopathies in 224 juvenile dogs.J Vet Intern Med. 2024 May-Jun;38(3):1598-1607. doi: 10.1111/jvim.17045. Epub 2024 Mar 14. J Vet Intern Med. 2024. PMID: 38483074 Free PMC article.
-
Conditions of the thoracolumbar spine.Semin Vet Med Surg Small Anim. 1996 Nov;11(4):235-53. doi: 10.1016/s1096-2867(96)80017-x. Semin Vet Med Surg Small Anim. 1996. PMID: 9020577 Review.
-
Common Neurologic Diseases in Geriatric Dogs.Animals (Basel). 2024 Jun 10;14(12):1753. doi: 10.3390/ani14121753. Animals (Basel). 2024. PMID: 38929372 Free PMC article. Review.
Cited by
-
Lumbar round cell sarcoma in a 10-week-old rottweiler puppy.Acta Vet Scand. 2025 Mar 12;67(1):12. doi: 10.1186/s13028-025-00800-1. Acta Vet Scand. 2025. PMID: 40075489 Free PMC article.
-
Demographics, clinical findings and diagnoses of cranial thoracic myelopathies (T1-T6 vertebrae) in cats.J Feline Med Surg. 2023 Oct;25(10):1098612X231199731. doi: 10.1177/1098612X231199731. J Feline Med Surg. 2023. PMID: 37791892 Free PMC article.
-
Comparison of Clinical Features of Intervertebral Disc Extrusions in English Cocker Spaniels, French Bulldogs and Dachshunds.Animals (Basel). 2025 Feb 19;15(4):602. doi: 10.3390/ani15040602. Animals (Basel). 2025. PMID: 40003082 Free PMC article.
References
-
- De Lahunta A, Glass E, Kent M. Neuroanatomy gross description and atlas of transverse sections and magnetic resonance images. In: De Lahunta A, Glass E, Kent M, editors. De Lahunta's Veterinary Neuroanatomy and Clinical Neurology. 5th ed. Philadelphia, PA: Elsevier, Inc. (2021). p. 6–44.
-
- De Lahunta A, Glass E, Kent M. Small animal spinal cord disease. In: De Lahunta A, Glass E, Kent M, editors. De Lahunta's Veterinary Neuroanatomy and Clinical Neurology. 5th ed. Philadelphia, PA: Elsevier, Inc. (2021). p. 267–311.
-
- De Lahunta A, Glass E, Kent M. Lower motor neuron: general visceral efferent system. In: De Lahunta A, Glass E, Kent M, editors. De Lahunta's Veterinary Neuroanatomy and Clinical Neurology. 5th ed. Philadelphia, PA: Elsevier, Inc. (2021). p. 203–29.
LinkOut - more resources
Full Text Sources