

A Distributed Cancer Care Model with a Technology-Driven Hub-and-Spoke and further Spoke Hierarchy: Findings from a Pilot Implementation Programme in Kerala, India
- PMID: 36172676
- PMCID: PMC9810301
- DOI: 10.31557/APJCP.2022.23.9.3133
A Distributed Cancer Care Model with a Technology-Driven Hub-and-Spoke and further Spoke Hierarchy: Findings from a Pilot Implementation Programme in Kerala, India
Abstract
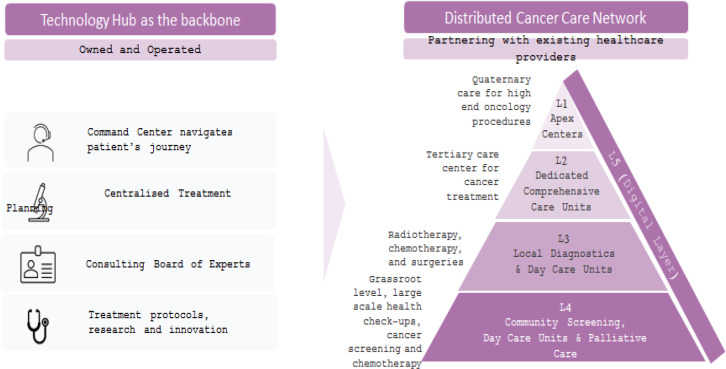
Background: The technology enabled distributed model in Kerala is based on an innovative partnership model between Karkinos Healthcare and private health centers. The model is designed to address the barriers to cancer screening by generating demand and by bringing together the private health centers and service providers at various levels to create a network for continued care. This paper describes the implementation process and presents some preliminary findings. Methods: The model follows the hub-and-spoke and further spoke framework. In the pilot phases, from July 2021 to December 2021, five private health centers (partners) collaborated with Karkinos Healthcare across two districts in Kerala. Screening camps were organized across the districts at the community level where the target groups were administered a risk assessment questionnaire followed by screening tests at the spoke hospitals based on a defined clinical protocol. The screened positive patients were examined further for confirmatory diagnosis at the spoke centers. Patients requiring chemotherapy or minor surgeries were treated at the spokes. For radiation therapy and complex surgeries the patients were referred to the hubs.
Results: A total of 2,459 individuals were screened for cancer at the spokes and 299 were screened positive. Capacity was built at the spokes for cancer surgery and chemotherapy. A total of 189 chemotherapy sessions and 17 surgeries were performed at the spokes for cancer patients. 70 patients were referred to the hub.
Conclusion: Initial results demonstrate the ability of the technology Distributed Cancer Care Network (DCCN) system to successfully screen and detect cancer and to converge the actions of various private health facilities towards providing a continuum of cancer care. The lessons learnt from this study will be useful for replicating the process in other States.
Keywords: COVID-19; India; access; cancer; technology.
Conflict of interest statement
No potential conflict of interest declared.
Figures
Similar articles
-
Role of digital health in coordinating patient care in a hub-and-spoke hierarchy of cancer care facilities: a scoping review.Ecancermedicalscience. 2023 Sep 25;17:1605. doi: 10.3332/ecancer.2023.1605. eCollection 2023. Ecancermedicalscience. 2023. PMID: 37799945 Free PMC article.
-
Mortality Following Diagnosis of Nontraumatic Intracerebral Hemorrhage Within an Integrated "Hub-and-Spoke" Neuroscience Care Model: Is Spoke Presentation Noninferior to Hub Presentation?Neurocrit Care. 2023 Jun;38(3):761-770. doi: 10.1007/s12028-022-01667-0. Epub 2023 Jan 4. Neurocrit Care. 2023. PMID: 36600074
-
Accessing perinatal substance use disorder care in your local community: A case study of an innovative hub and spoke network in western North Carolina.J Subst Use Addict Treat. 2024 Mar;158:209268. doi: 10.1016/j.josat.2023.209268. Epub 2023 Dec 12. J Subst Use Addict Treat. 2024. PMID: 38097044
-
Strengthening cardiac services in Faridabad District: A facility mapping exercise to explore implementation of a hub-and-spoke model.Indian J Med Res. 2024 Mar & Apr;159(3 & 4):347-355. doi: 10.25259/IJMR_1789_23. Indian J Med Res. 2024. PMID: 39361799 Free PMC article.
-
Healthcare stakeholders' perceptions and experiences of factors affecting the implementation of critical care telemedicine (CCT): qualitative evidence synthesis.Cochrane Database Syst Rev. 2021 Feb 18;2(2):CD012876. doi: 10.1002/14651858.CD012876.pub2. Cochrane Database Syst Rev. 2021. PMID: 33599282 Free PMC article.
Cited by
-
A practical approach for adoption of a hub and spoke model for cell and gene therapies in low- and middle-income countries: framework and case studies.Gene Ther. 2024 Jan;31(1-2):1-11. doi: 10.1038/s41434-023-00425-x. Epub 2023 Oct 30. Gene Ther. 2024. PMID: 37903929 Free PMC article. Review.
-
Factors Associated With Default of Treatment and Follow-Up Among Patients With Cancer: A Cross-Sectional Study From a Lower-Middle-Income Country.JCO Glob Oncol. 2024 Oct;10:e2400411. doi: 10.1200/GO-24-00411. Epub 2024 Nov 7. JCO Glob Oncol. 2024. PMID: 39509662 Free PMC article.
-
Role of digital health in coordinating patient care in a hub-and-spoke hierarchy of cancer care facilities: a scoping review.Ecancermedicalscience. 2023 Sep 25;17:1605. doi: 10.3332/ecancer.2023.1605. eCollection 2023. Ecancermedicalscience. 2023. PMID: 37799945 Free PMC article.
References
-
- Adab P, McGhee SM, Yanova J, Wong CM, Hedley AJ. Effectiveness and efficiency of opportunistic cervical cancer screening comparison with organized screening. Med Care. 2004;42:600–9. - PubMed
-
- Bretthauer M, Kalager M. Principles, effectiveness and caveats in screening for cancer. Br J Surg. 2013;100:55–65. - PubMed
-
- Dsouza NDR, Murthy NS, Aras RY. Projection of burden of cancer mortality for india, 2011-2026. Asian Pac J Cancer Prev. 2013a;14:4387–92. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical