

The Impact of Baseline User Characteristics on the Benefits of Real-Time Versus Intermittently Scanned Continuous Glucose Monitoring in Adults With Type 1 Diabetes: Moderator Analyses of the ALERTT1 Trial
- PMID: 36172693
- PMCID: PMC11089880
- DOI: 10.1177/19322968221128315
The Impact of Baseline User Characteristics on the Benefits of Real-Time Versus Intermittently Scanned Continuous Glucose Monitoring in Adults With Type 1 Diabetes: Moderator Analyses of the ALERTT1 Trial
Abstract
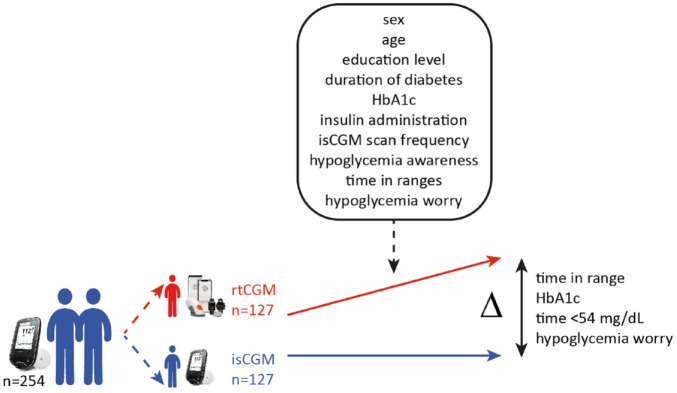
Background: ALERTT1 showed that switching from intermittently scanned continuous glucose monitoring (isCGM) without alerts to real-time CGM (rtCGM) with alert functionality improved time in range (TIR; 70-180 mg/dL), glycated hemoglobin (HbA1c), time <54 mg/dL, and Hypoglycemia Fear Survey version II worry subscale (HFS-worry) score after six months in adults with type 1 diabetes (T1D). Moderator analyses aimed to identify certain subgroups that would benefit more from switching to rtCGM than others.
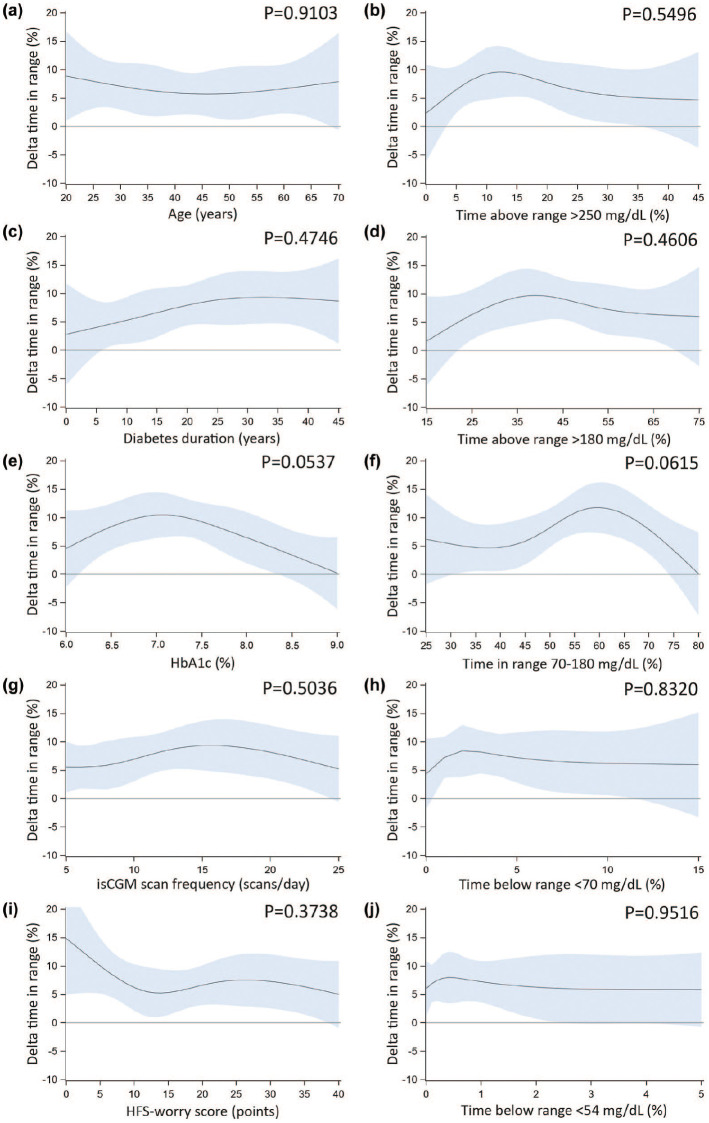
Methods: Post hoc analyses of ALERTT1 evaluated the impact of 14 baseline characteristics on the difference (delta) in mean TIR, HbA1c, time <54 mg/dL, and HFS-worry score at six months between rtCGM and isCGM. Therefore, the delta was allowed to depend on each of these variables by including interactions in the moderator analysis model. Analyses were performed separately for each variable; variables with P < .10 in the univariable analysis were combined into a single model.
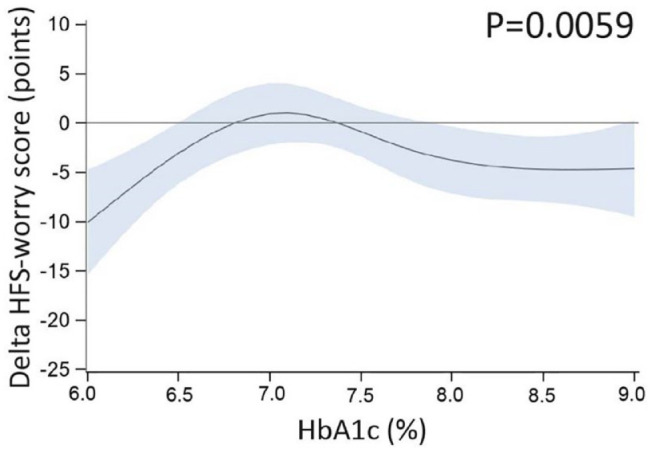
Results: Univariable analyses showed no dependency of delta TIR, HbA1c, or time <54 mg/dL on variables other than CGM type. Only delta HFS-worry score depended on baseline HbA1c (P = .0059), indicating less worries with rtCGM in people with baseline HbA1c <6.5% or ≥8%. Given P < .10 for dependency of delta TIR on insulin therapy type (favoring multiple daily injections), baseline HbA1c, and baseline TIR, these variables were combined into a multivariable analysis; interactions were not statistically significant.
Conclusions: Except for HFS-worry score, no interactions between 14 baseline characteristics and the six-month intervention effect of rtCGM on TIR, HbA1c, or time <54 mg/dL were observed, supporting the conclusion of ALERTT1 that switching from isCGM without alerts to rtCGM with alert functionality is beneficial for a wide range of people with T1D.
Keywords: continuous glucose monitoring; intermittently scanned continuous glucose monitoring; moderator analysis; real-time continuous glucose monitoring; type 1 diabetes.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: UZ Leuven received nonfinancial support for travel from Novo Nordisk, and Boehringer-Ingelheim for M.M.V. M.M.V. serves or has served on the speakers bureau for Dexcom—financial compensation for these activities has been received by KU Leuven. KU Leuven received nonfinancial support for travel from Medtronic, and financial support for travel from Roche for S.C. C.D.B. reports consulting fees and honoraria for speaking for Abbott, AstraZeneca, Boehringer-Ingelheim, A. Menarini Diagnostics, Eli Lilly, Medtronic, Novo Nordisk, and Roche. R.H. serves or has served on the advisory panel for Merck Sharp and Dohme, Boehringer-Ingelheim, and Eli Lilly. L.V.H. reports consulting fees and honoraria for speaking for Abbott, AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Medtronic, Merck Sharp and Dohme, Novo Nordisk, and Sanofi-Aventis. G.V. serves or has served on the advisory panel for Merck Sharp and Dohme, Boehringer-Ingelheim, and Eli Lilly. G.V. reports consulting fees and honoraria for speaking from Merck Sharp and Dohme, Boehringer-Ingelheim, AstraZeneca, Sanofi-Aventis, Novo Nordisk, and Eli Lilly. E.D. has served on the advisory panel for Novo Nordisk. E.D. reports speaking fees from Novo Nordisk, Boehringer-Ingelheim, Eli Lilly, and AstraZeneca. N.M. serves or has served on the advisory panel for Boehringer-Ingelheim. N.M. reports speaking fees from Merck Sharp and Dohme, Boehringer-Ingelheim, AstraZeneca, Sanofi-Aventis, Novo Nordisk, and Eli Lilly. C.V. reports consulting and speaking fees from Medtronic, Boehringer-Ingelheim, AstraZeneca, and Sanofi-Aventis. F.N. reports consulting fees and honoraria for speaking from Abbott, AstraZeneca, Boehringer-Ingelheim, Eli Lilly, Johnson and Johnson, Medtronic, Merck Sharp and Dohme, Novo Nordisk, Roche, and Sanofi-Aventis. C.M. serves or has served on the advisory panel for Novo Nordisk, Sanofi-Aventis, Merck Sharp and Dohme, Eli Lilly, Novartis, AstraZeneca, Boehringer-Ingelheim, Roche, Medtronic, ActoBio Therapeutics, Pfizer, and Zealand Pharma. Financial compensation for these activities has been received by KU Leuven; KU Leuven has received research support for C.M. from Medtronic, Novo Nordisk, Sanofi-Aventis, Merck Sharp and Dohme, Eli Lilly, Roche, Abbott, ActoBio Therapeutics, and Novartis; C.M. serves or has served on the speakers bureau for Novo Nordisk, Sanofi-Aventis, Merck Sharp and Dohme, Eli Lilly, Boehringer-Ingelheim, AstraZeneca, and Novartis. Financial compensation for these activities has been received by KU Leuven. P.G. serves or has served on the advisory panel for Novo Nordisk, Sanofi-Aventis, Boehringer-Ingelheim, Janssen Pharmaceuticals, Roche, Medtronic, and Bayer. Financial compensation for these activities has been received by KU Leuven. P.G. serves or has served on the speakers bureau for Merck Sharp and Dohme, Boehringer-Ingelheim, Bayer, Medtronic, Insulet, Novo Nordisk, Abbott, Roche, and Dexcom. Financial compensation for these activities has been received by KU Leuven. KU Leuven received nonfinancial support for travel from Sanofi-Aventis, A. Menarini Diagnostics, Medtronic, and Roche for P.G. All disclosures were unrelated to the present work. S.F., T.M., and B.K. have nothing to disclose.
Figures
Similar articles
-
Comparing real-time and intermittently scanned continuous glucose monitoring in adults with type 1 diabetes (ALERTT1): a 6-month, prospective, multicentre, randomised controlled trial.Lancet. 2021 Jun 12;397(10291):2275-2283. doi: 10.1016/S0140-6736(21)00789-3. Epub 2021 Jun 2. Lancet. 2021. PMID: 34089660 Clinical Trial.
-
Effect of switching from intermittently scanned to real-time continuous glucose monitoring in adults with type 1 diabetes: 24-month results from the randomised ALERTT1 trial.Lancet Diabetes Endocrinol. 2023 Feb;11(2):96-108. doi: 10.1016/S2213-8587(22)00352-7. Lancet Diabetes Endocrinol. 2023. PMID: 36702566 Clinical Trial.
-
Switching from Intermittently Scanned Continuous Glucose Monitoring to Real-Time Continuous Glucose Monitoring with a Predictive Urgent Low Soon Alert Reduces Exposure to Hypoglycemia.Diabetes Technol Ther. 2024 Jul;26(7):498-502. doi: 10.1089/dia.2023.0434. Epub 2024 Apr 9. Diabetes Technol Ther. 2024. PMID: 38315504
-
Comparing the glycaemic outcomes between real-time continuous glucose monitoring (rt-CGM) and intermittently scanned continuous glucose monitoring (isCGM) among adults and children with type 1 diabetes: A systematic review and meta-analysis of randomized controlled trials.Diabet Med. 2024 Mar;41(3):e15280. doi: 10.1111/dme.15280. Epub 2024 Jan 10. Diabet Med. 2024. PMID: 38197238
-
Glucose Targets Using Continuous Glucose Monitoring Metrics in Older Adults With Diabetes: Are We There Yet?J Diabetes Sci Technol. 2024 Jul;18(4):808-818. doi: 10.1177/19322968241247568. Epub 2024 May 7. J Diabetes Sci Technol. 2024. PMID: 38715259 Free PMC article. Review.
Cited by
-
Utility and precision evidence of technology in the treatment of type 1 diabetes: a systematic review.Commun Med (Lond). 2023 Oct 5;3(1):132. doi: 10.1038/s43856-023-00358-x. Commun Med (Lond). 2023. PMID: 37794113 Free PMC article.
References
-
- Bolinder J, Antuna R, Geelhoed-Duijvestijn P, Kröger J, Weitgasser R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: a multicentre, nonmasked, randomised controlled trial. Lancet. 2016;388: 2254-2263. - PubMed
-
- Tumminia A, Crimi S, Sciacca L, et al.. Efficacy of real-time continuous glucose monitoring on glycaemic control and glucose variability in type 1 diabetic patients treated with either insulin pumps or multiple insulin injection therapy: a randomized controlled crossover trial. Diabetes Metab Res Rev. 2015;31(1):61-68. - PubMed
-
- van Beers CA, DeVries JH, Kleijer SJ, et al.. Continuous glucose monitoring for patients with type 1 diabetes and impaired awareness of hypoglycaemia (IN CONTROL): a randomised, open-label, crossover trial. Lancet Diabetes Endocrinol. 2016;4(11):893-902. - PubMed
-
- Lind M, Polonsky W, Hirsch IB, et al.. Continuous glucose monitoring vs conventional therapy for glycemic control in adults with type 1 diabetes treated with multiple daily insulin injections the GOLD randomized clinical trial. JAMA. 2017;317:379-387. - PubMed
-
- Beck RW, Riddlesworth T, Ruedy K, et al.. Effect of continuous glucose monitoring on glycemic control in adults with type 1 diabetes using insulin injections the DIAMOND randomized clinical trial. JAMA. 2017;317:371-378. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
