

Clinical Practice Variations in the Management of Ischemia With No Obstructive Coronary Artery Disease
- PMID: 36172938
- PMCID: PMC9673699
- DOI: 10.1161/JAHA.121.022573
Clinical Practice Variations in the Management of Ischemia With No Obstructive Coronary Artery Disease
Abstract
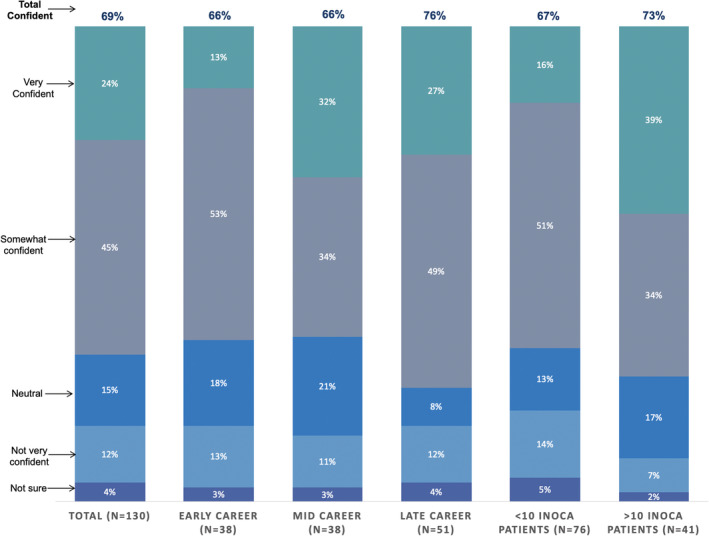
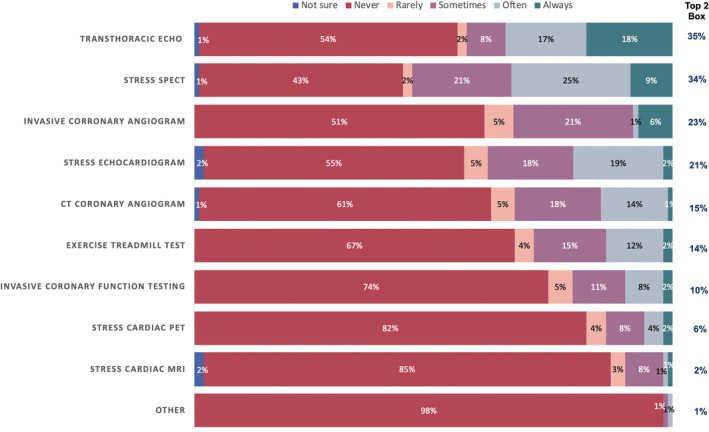
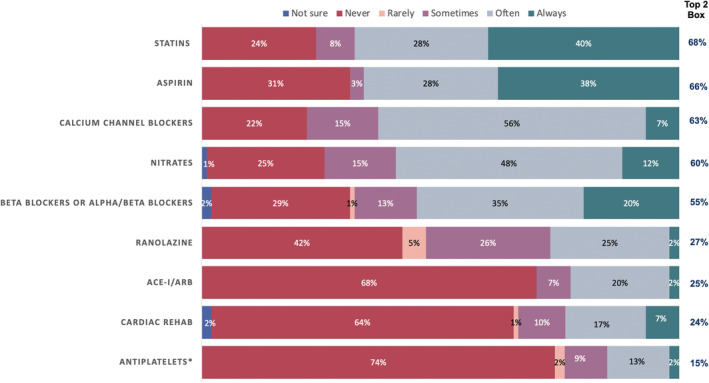
Background Ischemia with no obstructive coronary artery disease is a condition associated with major adverse cardiovascular outcomes. To date, there are no specific American Heart Association or American College of Cardiology guidelines. The objective of this survey is to better understand the clinical practice and knowledge gaps that exist nationally. Methods and Results Participant-specific links for a survey with 11 questions and 3 reminders were sent between September and October 2020 to the American College of Cardiology CardioSurve Panel. The panel consist of randomly selected cardiologists (n=437) who represent the current profile of the American College of Cardiology US membership. The survey received a 30% response rate. Of the 172 respondents, 130 (76%) indicated that they have treated patients with ischemia with no obstructive coronary artery disease. Although the majority (69%) are generally confident in their ability to manage this condition, 1 of 3 report lack of confidence or are neutral. The American College of Cardiology/American Heart Association Chronic Stable Angina Guidelines are the most commonly used reference for treating ischemia with no obstructive coronary artery disease (81%), with most cardiologists wanting additional clinical guidance, such as randomized controlled trials (61%). More than 4 of 5 cardiologists rarely or never order advanced imaging modalities to assess coronary flow reserve. Approximately 2 of 3 of respondents frequently prescribe statins (68%), aspirin (66%), calcium channel blockers (63%), and β blockers or α/β blockers (55%). However, nearly 70% never prescribe angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. Conclusions This survey demonstrates heterogeneity in the management of ischemia with no obstructive coronary artery disease among US cardiologists, identifies support for guideline development, and outlines knowledge gaps for research and education in the therapeutic management of this condition.
Keywords: angina; guidelines; ischemia with no obstructive coronary arteries; ischemic heart disease; nonobstructive; stable coronary syndromes.
Figures
Similar articles
-
Sex Differences in Cardiac Medication Use Post-Catheterization in Patients Undergoing Coronary Angiography for Stable Angina with Nonobstructive Coronary Artery Disease.J Womens Health (Larchmt). 2017 Sep;26(9):976-983. doi: 10.1089/jwh.2016.5983. Epub 2017 Apr 6. J Womens Health (Larchmt). 2017. PMID: 28384013
-
Cardiac Medication Use in Patients with Acute Myocardial Infarction and Nonobstructive Coronary Artery Disease.J Womens Health (Larchmt). 2017 Nov;26(11):1185-1192. doi: 10.1089/jwh.2016.5984. Epub 2017 Apr 6. J Womens Health (Larchmt). 2017. PMID: 28384014
-
Current treatment of hypertension in patients with coronary artery disease recommended by different guidelines.Expert Opin Pharmacother. 2016;17(2):205-15. doi: 10.1517/14656566.2015.1091881. Epub 2015 Sep 16. Expert Opin Pharmacother. 2016. PMID: 26373919 Review.
-
Utilization of secondary prevention therapies in patients with nonobstructive coronary artery disease identified during cardiac catheterization: insights from the National Cardiovascular Data Registry Cath-PCI Registry.Circ Cardiovasc Qual Outcomes. 2010 Nov;3(6):632-41. doi: 10.1161/CIRCOUTCOMES.109.906214. Epub 2010 Oct 5. Circ Cardiovasc Qual Outcomes. 2010. PMID: 20923997
-
Conventional and novel drug therapeutics to relief myocardial ischemia.Cardiovasc Drugs Ther. 2010 Aug;24(4):319-23. doi: 10.1007/s10557-010-6254-8. Cardiovasc Drugs Ther. 2010. PMID: 20658184 Review.
Cited by
-
Endothelial cell dysfunction in cardiac disease: driver or consequence?Front Cell Dev Biol. 2023 Oct 25;11:1278166. doi: 10.3389/fcell.2023.1278166. eCollection 2023. Front Cell Dev Biol. 2023. PMID: 37965580 Free PMC article. Review.
-
Diagnostic accuracy of non-invasive investigations for coronary artery disease in hypertensive patients: a meta-analysis.Arch Med Sci. 2024 Jun 6;21(1):167-178. doi: 10.5114/aoms/188782. eCollection 2025. Arch Med Sci. 2024. PMID: 40190327 Free PMC article. Review.
-
Use of machine learning to identify risk factors for coronary artery disease.PLoS One. 2023 Apr 14;18(4):e0284103. doi: 10.1371/journal.pone.0284103. eCollection 2023. PLoS One. 2023. PMID: 37058460 Free PMC article.
-
[Diagnosis and treatment of patients with ANOCA. Consensus document of the SEC-Clinical Cardiology Association/SEC-Interventional Cardiology Association/SEC-Ischemic Heart Disease and Acute Cardiac Care Association/ SEC-Cardiovascular Imaging Association].REC Interv Cardiol. 2023 Dec 20;6(2):106-116. doi: 10.24875/RECIC.M23000422. eCollection 2024 Apr-Jun. REC Interv Cardiol. 2023. PMID: 40416348 Free PMC article. Spanish.
References
-
- Jespersen L, Hvelplund A, Abildstrøm SZ, Pedersen F, Galatius S, Madsen JK, Jørgensen E, Kelbæk H, Prescott E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734–744. doi: 10.1093/eurheartj/ehr331 - DOI - PubMed
-
- Blumgart HL, Schlesinger MJ, Davis D. Studies on the relation of the clinical manifestations of angina pectoris, coronary thrombosis, and myocardial infarction to the pathologic findings: with particular reference to the significance of the collateral circulation. Am Heart J. 1940;19:1–91. doi: 10.1016/S0002-8703(40)90305-2 - DOI
-
- Mehta P, Wei J, Bairey Merz N. Chapter 25: angina in patients with evidence of myocardial ischemia and no obstructive coronary artery disease. In: Braunwald E, ed. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 10th ed. Philadelphia, Pa: Elsevier/Saunders; 2014.
-
- Ford TJ, Yii E, Sidik N, Good R, Rocchiccioli P, McEntegart M, Watkins S, Eteiba H, Shaukat A, Lindsay M, et al. Ischemia and no obstructive coronary artery disease: prevalence and correlates of coronary vasomotion disorders. Circ Cardiovasc Interv. 2019;12:e008126. doi: 10.1161/CIRCINTERVENTIONS.119.008126 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
