

Botulinum toxin A for management of refractory concurrent buccal and inferior alveolar nerve post-traumatic neuropathies: a case report
- PMID: 36172992
- PMCID: PMC9528003
- DOI: 10.1177/03000605211047704
Botulinum toxin A for management of refractory concurrent buccal and inferior alveolar nerve post-traumatic neuropathies: a case report
Abstract
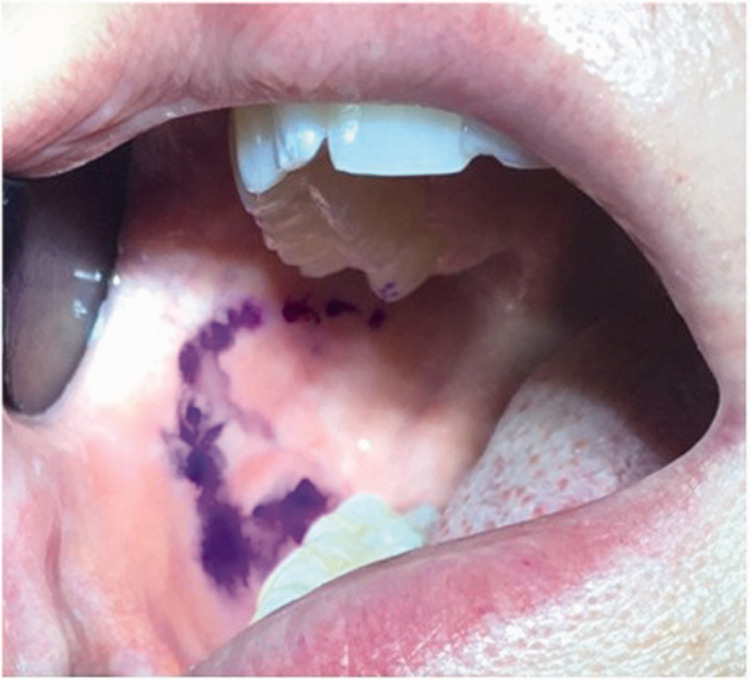
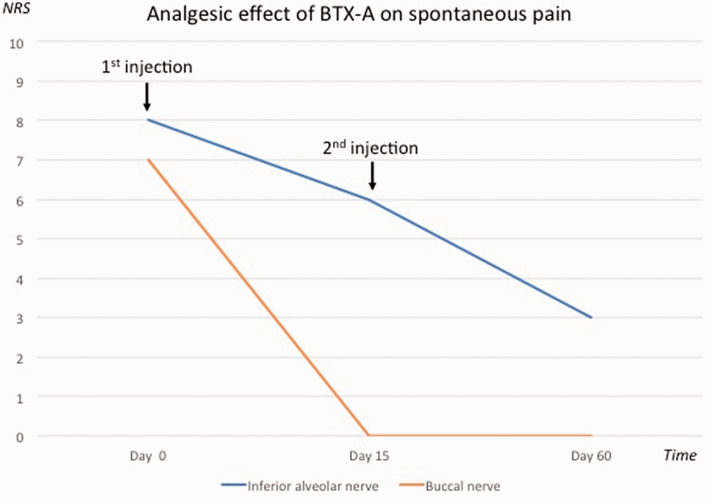
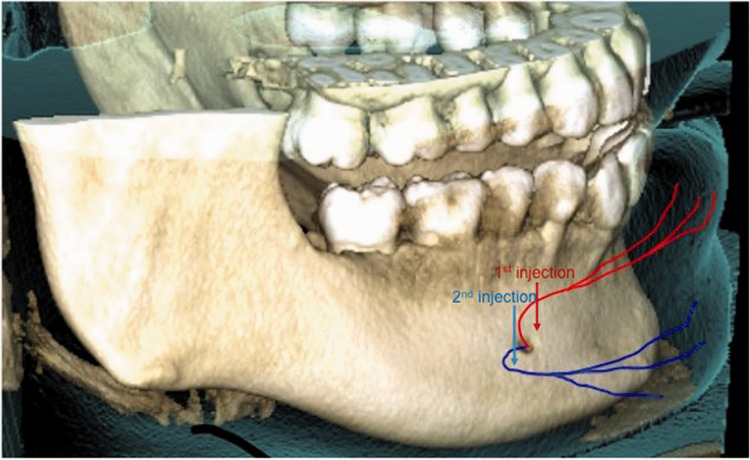
Painful post-traumatic trigeminal neuropathy (PPTTN) can result from iatrogenic injury to one or more branches of the trigeminal nerve during oral surgical procedures such as tooth extractions. Like other chronic neuropathic pain conditions, PPTTN can significantly alter the patient's quality of life, especially when pharmacological treatment is ineffective or not tolerated. As such, new treatment options have been investigated, including local injections of botulinum toxin type A (BTX-A). A 29-year-old woman presented to our tertiary orofacial pain clinic for evaluation of chronic electric shock-like pain attacks and severe allodynia in the territory of the right inferior alveolar nerve and buccal nerve following right mandibular third molar extraction 3 years prior. Following several failed attempts at classic pharmacological management (including carbamazepine, venlafaxine, duloxetine, pregabalin, clonazepam, and amitriptyline), BTX-A injections were administered in the vicinity of the right mental nerve. This treatment provided significant improvement in the patient's condition and overall quality of life with no significant adverse effects. Because both neuropathies were significantly improved by remote BTX-A injections, this case report provides preliminary clinical evidence supporting spinopetal transport of BTX-A, as shown in animal models, as an underlying pathophysiological mechanism of BTX-A-mediated analgesia.
Keywords: Painful post-traumatic trigeminal neuropathy; botulinum toxin type A; buccal nerve; facial pain; inferior alveolar nerve; spinopetal transport.
Conflict of interest statement
Figures

Similar articles
-
Topical Review: Potential Use of Botulinum Toxin in the Management of Painful Posttraumatic Trigeminal Neuropathy.J Oral Facial Pain Headache. 2017 Winter;31(1):7-18. doi: 10.11607/ofph.1753. J Oral Facial Pain Headache. 2017. PMID: 28118416 Review.
-
[Botulinum toxin and painful peripheral neuropathies: what should be expected?].Rev Neurol (Paris). 2011 Jan;167(1):46-50. doi: 10.1016/j.neurol.2010.11.001. Epub 2010 Dec 30. Rev Neurol (Paris). 2011. PMID: 21194720 Review. French.
-
Neuromodulators for Atypical Facial Pain and Neuralgias: A Systematic Review and Meta-Analysis.Laryngoscope. 2021 Jun;131(6):1235-1253. doi: 10.1002/lary.29162. Epub 2020 Oct 10. Laryngoscope. 2021. PMID: 33037835
-
Botulinum Toxin Type A for the Treatment of Neuropathic Pain in Neuro-Rehabilitation.Toxins (Basel). 2015 Jun 30;7(7):2454-80. doi: 10.3390/toxins7072454. Toxins (Basel). 2015. PMID: 26134256 Free PMC article. Review.
-
Onabotulinum toxin a treatment for posttraumatic trigeminal neuropathic pain: case series and literature review.J Oral Facial Pain Headache. 2024 Mar;38(1):93-105. doi: 10.22514/jofph.2024.009. Epub 2024 Mar 12. J Oral Facial Pain Headache. 2024. PMID: 39788579 Free PMC article. Review.
Cited by
-
Effectiveness of Botulinum Toxin in the Treatment of Neuropathic Pain: A Literature Review.Cureus. 2023 Oct 11;15(10):e46848. doi: 10.7759/cureus.46848. eCollection 2023 Oct. Cureus. 2023. PMID: 37954779 Free PMC article. Review.
-
Clinical insights into traumatic injury of the inferior alveolar and lingual nerves: a comprehensive approach from diagnosis to therapeutic interventions.Clin Oral Investig. 2024 Mar 15;28(4):216. doi: 10.1007/s00784-024-05615-4. Clin Oral Investig. 2024. PMID: 38488908 Free PMC article. Review.
-
Buccal neuralgia: a potential cause of facial pain.Neurol Sci. 2025 Apr 24. doi: 10.1007/s10072-025-08201-y. Online ahead of print. Neurol Sci. 2025. PMID: 40272747 No abstract available.
References
-
- Headache classification committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018; 38: 1–211. doi: 10.1177/0333102417738202. - PubMed
-
- Benoliel R, Kahn J, Eliav E. Peripheral painful traumatic trigeminal neuropathies. Oral Dis 2012; 18: 317–332. doi: 10.1111/j.1601-0825.2011.01883. - PubMed
-
- O’Connor AB. Neuropathic pain: Quality-of-life impact, costs and cost effectiveness of therapy. Pharmacoeconomics 2009; 27: 95–112. doi: 10.2165/00019053-200927020-00002. - PubMed
-
- Renton T, Yilmaz Z. Profiling of patients presenting with posttraumatic neuropathy of the trigeminal nerve. J Orofac Pain 2011; 25: 333–344. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
