

Novel anatomical findings with implications on the etiology of the piriformis syndrome
- PMID: 36173479
- PMCID: PMC9649478
- DOI: 10.1007/s00276-022-03023-5
Novel anatomical findings with implications on the etiology of the piriformis syndrome
Abstract
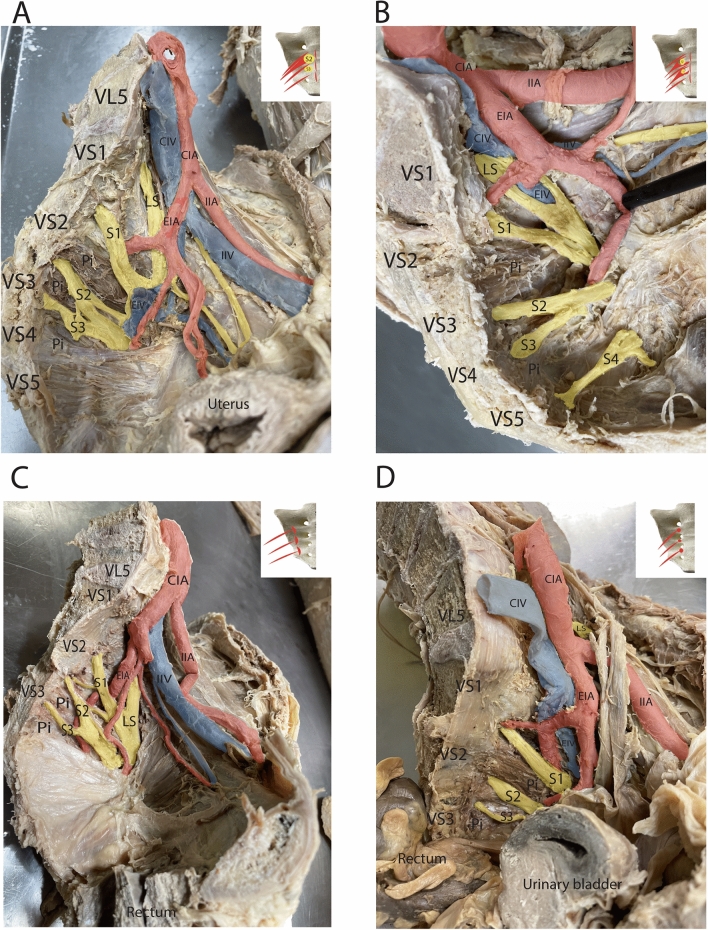
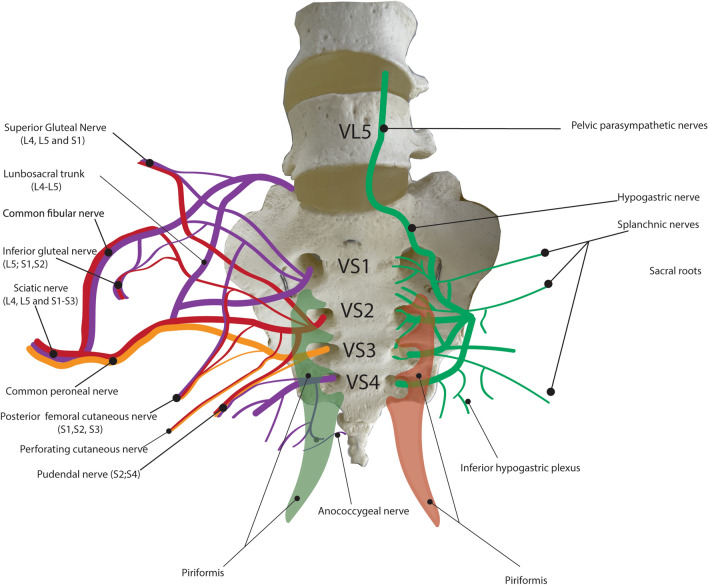
Purpose: The cause of the piriformis-related pelvic and extra-pelvic pain syndromes is still not well understood. Usually, the piriformis syndrome is seen as extra-pelvic sciatica caused by the entrapment of the sciatic nerve by the piriformis in its crossing through the greater sciatic foramen. However, the piriformis muscle may compress additional nerve structures in other regions and cause idiotypic pelvic pain, pelvic visceral pain, pudendal neuralgia, and pelvic organ dysfunction. There is still a lack of detailed description of the muscle origin, topography, and its possible relationships with the anterior branches of the sacral spinal nerves and with the sacral plexus. In this research, we aimed to characterize the topographic relationship of the piriformis with its surrounding anatomical structures, especially the anterior branches of the sacral spinal nerves and the sacral plexus in the pelvic cavity, as well as to estimate the possible role of anatomical piriformis variants in pelvic pain and extra-pelvic sciatica.
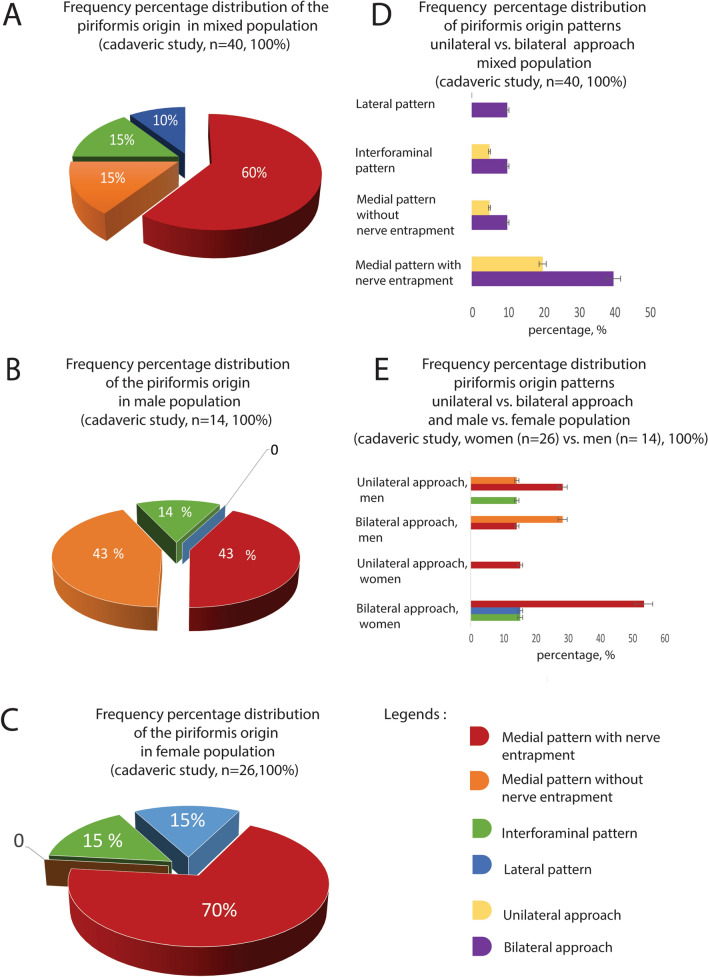
Methods: Human cadaveric material was used accordingly to the Swiss Academy of Medical Science Guidelines adapted in 2021 and the Federal Act on Research involving Human Beings (Human Research ACT, HRA, status as 26, May 2021). All body donors gave written consent for using their bodies for teaching and research. 14 males and 26 females were included in this study. The age range varied from 64 to 97 years (mean 84 ± 10.7 years, median 88).
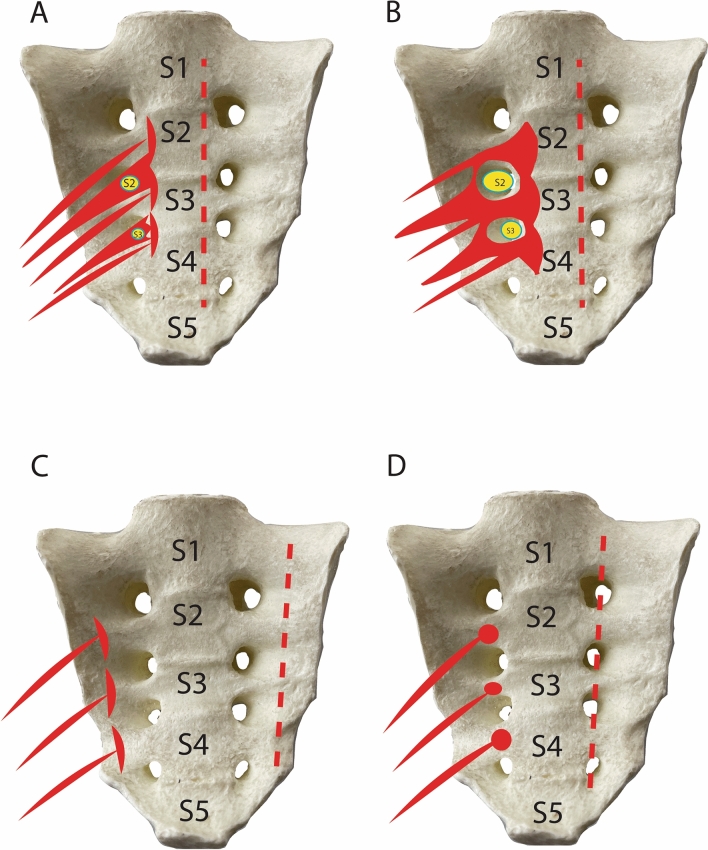
Results: three variants of the sacral origin of the piriformis were found when referring to the relationship between the muscle and the anterior sacral foramen. Firstly, the medial muscle origin pattern and its complete covering of the anterior sacral foramen by the piriformis muscle is the most frequent anatomical variation (43% in males, 70% in females), probably with the most relevant clinical impact. This pattern may result in the compression of the anterior branches of the sacral spinal nerves when crossing the muscle.
Conclusions: These new anatomical findings may provide a better understanding of the complex piriformis and pelvic pain syndromes due to compression of the sacral spinal nerves with their somatic or autonomous (parasympathetic) qualities when crossing the piriformis.
Keywords: Deep gluteal space problems and piriformis syndrome; Pelvic pain syndrome; Piriformis; Pudendal neuralgia; Sacral plexus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors have no relevant financial or non-financial interests to disclose.
Figures
Similar articles
-
The majority of piriformis muscles are innervated by the superior gluteal nerve.Clin Anat. 2019 Mar;32(2):282-286. doi: 10.1002/ca.23311. Epub 2018 Dec 21. Clin Anat. 2019. PMID: 30408241
-
Vascular Entrapment of Both the Sciatic and Pudendal Nerves Causing Persistent Sciatica and Pudendal Neuralgia.J Minim Invasive Gynecol. 2019 Feb;26(2):360-361. doi: 10.1016/j.jmig.2018.04.014. Epub 2018 Apr 24. J Minim Invasive Gynecol. 2019. PMID: 29702268
-
[Piriformis muscle syndrome: etiology, pathogenesis, clinical manifestations, diagnosis, differential diagnosis and therapy].Lijec Vjesn. 2013 Jan-Feb;135(1-2):33-40. Lijec Vjesn. 2013. PMID: 23607175 Review. Croatian.
-
Sciatica of nondisc origin and piriformis syndrome: diagnosis by magnetic resonance neurography and interventional magnetic resonance imaging with outcome study of resulting treatment.J Neurosurg Spine. 2005 Feb;2(2):99-115. doi: 10.3171/spi.2005.2.2.0099. J Neurosurg Spine. 2005. PMID: 15739520
-
Case report and review of the potential role of the Type A piriformis muscle in dynamic sciatic nerve entrapment variant of piriformis syndrome.Surg Radiol Anat. 2020 Oct;42(10):1237-1242. doi: 10.1007/s00276-020-02440-8. Epub 2020 Feb 28. Surg Radiol Anat. 2020. PMID: 32112284 Review.
Cited by
-
Morphologic and morphometric bilateral analysis and sexual dimorphism in sciatic nerves of adult cadaveric specimens in Uganda.BMC Musculoskelet Disord. 2025 Apr 29;26(1):422. doi: 10.1186/s12891-025-08641-9. BMC Musculoskelet Disord. 2025. PMID: 40301790 Free PMC article.
-
Effective mnemonic techniques for memorizing the peripheral nervous system: a focus on the brachial, lumbar, and sacral plexuses.Front Surg. 2025 Jun 13;12:1511451. doi: 10.3389/fsurg.2025.1511451. eCollection 2025. Front Surg. 2025. PMID: 40585481 Free PMC article.
-
An atypical inferior gluteal artery passing through the piriformis muscle.Surg Radiol Anat. 2024 Jan;46(1):59-64. doi: 10.1007/s00276-023-03256-y. Epub 2023 Oct 26. Surg Radiol Anat. 2024. PMID: 37884741
-
YouTube as a source of education on piriformis injection: a content, quality, and reliability analysis.BMC Med Educ. 2025 Apr 16;25(1):549. doi: 10.1186/s12909-025-07154-2. BMC Med Educ. 2025. PMID: 40241034 Free PMC article.
-
Competencies of Large Language Models About Piriformis Syndrome: Quality, Accuracy, Completeness, and Readability Study.HSS J. 2025 May 20:15563316251340697. doi: 10.1177/15563316251340697. Online ahead of print. HSS J. 2025. PMID: 40405920 Free PMC article.
References
-
- Anand N, Birch R, Collins P, Crossman A, Gleeson M, Smith A, Spratt J, Stringer M, Tubbs S, Wigley C, Wein A. Gray’s Anatomy: the anatomical basis of clinical practice. 40. Amsterdam: Elsevier; 2016.
-
- de Azevedo MP. Anorectal and pelvic floor pain syndromes. Anorectal Physiol. 2020 doi: 10.1007/978-3-030-43811-1_30. - DOI
-
- Barge AS, Barge SM, Barge SS. Sacroiliac joint pain-presenting as sciatica-a common differential diagnosis. J Evol Med Dent Sci. 2019;8:953–956. doi: 10.14260/jemds/2019/211. - DOI
-
- Beaton LE, Anson BJ. The sciatic nerve and the piriformis muscle: their interrelation a possible cause of coccygodynia. J Bone Joint Surg. 1938;20:686–688. doi: 10.1097/00401515-193820030-00012. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
