

Prescribing Characteristics Associated With Opioid Overdose Following Buprenorphine Taper
- PMID: 36173629
- PMCID: PMC9523505
- DOI: 10.1001/jamanetworkopen.2022.34168
Prescribing Characteristics Associated With Opioid Overdose Following Buprenorphine Taper
Abstract
Importance: Retention in buprenorphine therapy is associated with a lower risk of opioid overdose. Nevertheless, many patients discontinue treatment, and there is limited evidence to guide buprenorphine tapering.
Objective: To understand what prescribing characteristics are associated with opioid overdose following buprenorphine taper.
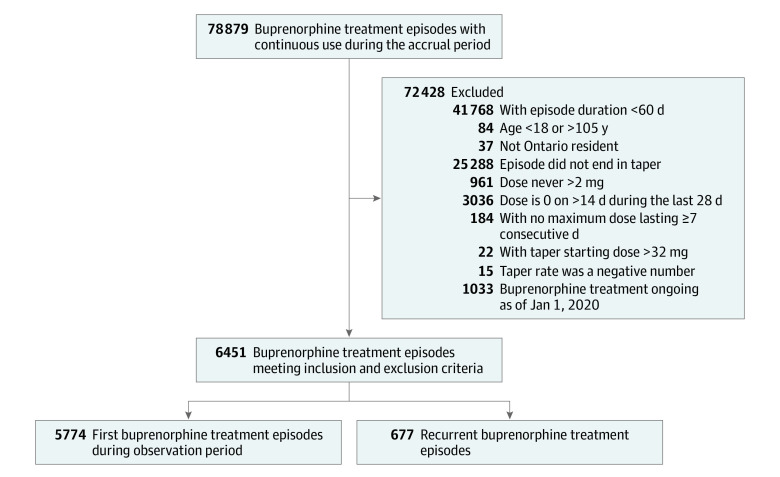
Design, setting, and participants: This is a population-based, retrospective, cohort study of adults who were maintained on buprenorphine for at least 60 days and underwent a buprenorphine taper. The study was conducted in the Canadian province of Ontario, using linked administrative health data. New buprenorphine treatment episodes were accrued between January 1, 2013, and January 1, 2019, and the maximum follow-up was April 30, 2020. Data analysis was performed from December 2020 to August 2022.
Exposures: The primary exposure of interest was time to taper initiation (≤1 year vs >1 year). Secondary exposures included mean rate of taper, percentage days during which the dose was decreasing, and taper duration.
Main outcomes and measures: The primary outcome measure was time to fatal or nonfatal opioid overdose within 18 months following treatment discontinuation.
Results: Among 5774 individuals, the median (IQR) age at index date was 34 (28-44) years, and 3462 individuals (60.0%) were male. Time to taper initiation longer than 1 year vs 1 year or less (6.73 vs 10.35 overdoses per 100 person-years; adjusted hazard ratio [aHR], 0.69; 95% CI, 0.48-0.997), a lower mean rate of taper (≤2 mg per month, 6.95 overdoses per 100 person-years; >2 to ≤4 mg per month, 11.48 overdoses per 100 person-years; >4 mg per month, 17.27 overdoses per 100 person-years; ≤2 mg per month vs >4 mg per month, aHR, 0.65; 95% CI, 0.46-0.91; >2 to ≤4 mg per month vs >4 mg per month, aHR, 0.69; 95% CI, 0.51-0.93), and dose decreases in 1.75% or less of days vs more than 3.50% of days during the taper period (5.87 vs 13.87 overdoses per 100 person-years; aHR, 0.64; 95% CI, 0.43-0.93) were associated with reduced risk of opioid overdose; however, taper duration was not.
Conclusions and relevance: In this retrospective cohort study, buprenorphine tapers undertaken after at least 1 year of therapy, a slower rate of taper, and a lower percentage of days during which the dose was decreasing were associated with a significantly lower risk of opioid overdose, regardless of taper duration. These findings underscore the importance of a carefully planned taper and could contribute to reduction in opioid-related overdose death.
Conflict of interest statement
Similar articles
-
Association Between Increased Dispensing of Opioid Agonist Therapy Take-Home Doses and Opioid Overdose and Treatment Interruption and Discontinuation.JAMA. 2022 Mar 1;327(9):846-855. doi: 10.1001/jama.2022.1271. JAMA. 2022. PMID: 35230394 Free PMC article.
-
The association between buprenorphine treatment duration and mortality: a multi-site cohort study of people who discontinued treatment.Addiction. 2023 Jan;118(1):97-107. doi: 10.1111/add.15998. Epub 2022 Jul 23. Addiction. 2023. PMID: 35815386 Free PMC article.
-
Duration of use and outcomes among people with opioid use disorder initiating methadone and buprenorphine in Ontario: a population-based propensity-score matched cohort study.Addiction. 2022 Jul;117(7):1972-1981. doi: 10.1111/add.15862. Epub 2022 Mar 21. Addiction. 2022. PMID: 35257434 Free PMC article.
-
Prior National Drug Abuse Treatment Clinical Trials Network (CTN) opioid use disorder trials as background and rationale for NIDA CTN-0100 "optimizing retention, duration and discontinuation strategies for opioid use disorder pharmacotherapy (RDD)".Addict Sci Clin Pract. 2021 Mar 6;16(1):15. doi: 10.1186/s13722-021-00223-z. Addict Sci Clin Pract. 2021. PMID: 33676577 Free PMC article. Review.
-
Opioid-related treatment, interventions, and outcomes among incarcerated persons: A systematic review.PLoS Med. 2019 Dec 31;16(12):e1003002. doi: 10.1371/journal.pmed.1003002. eCollection 2019 Dec. PLoS Med. 2019. PMID: 31891578 Free PMC article.
Cited by
-
What is the ideal time to begin tapering opioid agonist treatment? A protocol for a retrospective population-based comparative effectiveness study in British Columbia, Canada.BMJ Open. 2024 Apr 29;14(4):e083453. doi: 10.1136/bmjopen-2023-083453. BMJ Open. 2024. PMID: 38684262 Free PMC article.
-
Barriers to and facilitators of buprenorphine dispensing for opioid use disorder: Evidence from focus groups in Appalachian Kentucky.J Am Pharm Assoc (2003). 2025 Mar-Apr;65(2):102308. doi: 10.1016/j.japh.2024.102308. Epub 2024 Dec 4. J Am Pharm Assoc (2003). 2025. PMID: 39643270
-
Discontinuation of medication treatment for opioid use disorder after a successful course: The discontinuation phase of the CTN-0100 (RDD) trial.Contemp Clin Trials. 2024 Jul;142:107543. doi: 10.1016/j.cct.2024.107543. Epub 2024 Apr 23. Contemp Clin Trials. 2024. PMID: 38657730 Free PMC article. Clinical Trial.
-
Non-scheduled short-acting opioid to taper off opioids?CNS Neurosci Ther. 2024 Apr;30(4):e14705. doi: 10.1111/cns.14705. CNS Neurosci Ther. 2024. PMID: 38584343 Free PMC article.
-
Management of opioid use disorder: 2024 update to the national clinical practice guideline.CMAJ. 2024 Nov 11;196(38):E1280-E1290. doi: 10.1503/cmaj.241173. CMAJ. 2024. PMID: 39532476 Free PMC article.
References
-
- Government of Canada . Opioid and stimulant-related harms in Canada. 2021. Accessed March 7, 2022. https://health-infobase.canada.ca/substance-related-harms/opioids-stimul...
-
- Ahmad F, Rossen L, Sutton P. Provisional Drug Overdose Death Counts. National Center for Health Statistics; 2022.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
