

Evidence-based impact projections of single-dose human papillomavirus vaccination in India: a modelling study
- PMID: 36174583
- PMCID: PMC9622421
- DOI: 10.1016/S1470-2045(22)00543-5
Evidence-based impact projections of single-dose human papillomavirus vaccination in India: a modelling study
Abstract
Background: Despite the high burden of cervical cancer, access to preventive measures remains low in India. A single-dose immunisation schedule could facilitate the scale-up of human papillomavirus (HPV) vaccination, contributing to global elimination of cervical cancer. We projected the effect of single-dose quadrivalent HPV vaccination in India in comparison with no vaccination or to a two-dose schedule.
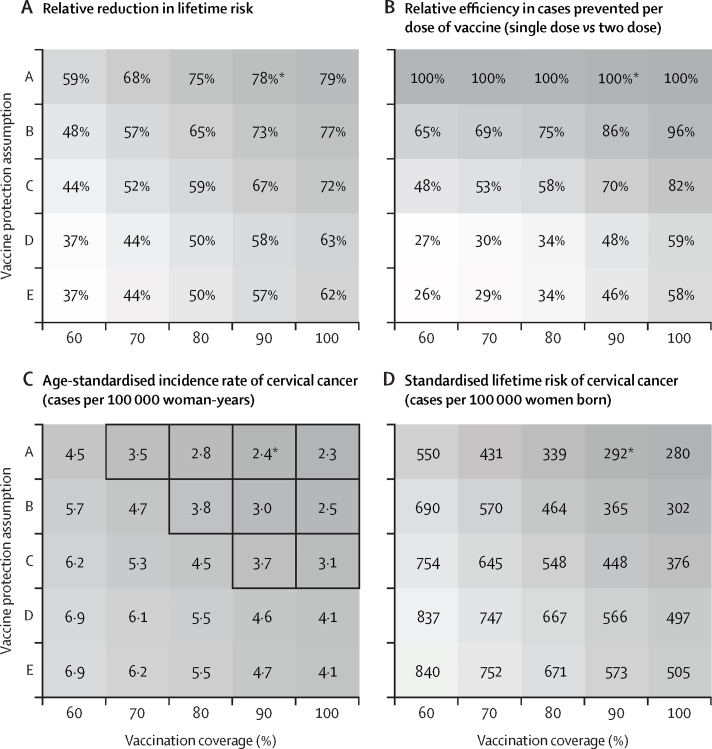
Methods: In this modelling study, we adapted an HPV transmission model (EpiMetHeos) to Indian data on sexual behaviour (from the Demographic and Health Survey and the Indian National AIDS Control Organisation), HPV prevalence data (from two local surveys, from the states of Tamil Nadu and West Bengal), and cervical cancer incidence data (from Cancer Incidence in Five Continents for the period 2008-12 [volume XI], and the Indian National Centre for Disease Informatics and Research for the period 2012-16). Using the model, we projected the nationwide and state-specific effect of HPV vaccination on HPV prevalence and cervical cancer incidence, and lifetime risk of cervical cancer, for 100 years after the introduction of vaccination or in the first 50 vaccinated birth cohorts. Projections were derived under a two-dose vaccination scenario assuming life-long protection and under a single-dose vaccination scenario with protection duration assumptions derived from International Agency for Research on Cancer (IARC) India vaccine trial data, in combination with different vaccination coverages and catch-up vaccination age ranges. We used two thresholds to define cervical cancer elimination: an age-standardised incidence rate of less than 4 cases per 100 000 woman-years, and standardised lifetime risk of less than 250 cases per 100 000 women born.
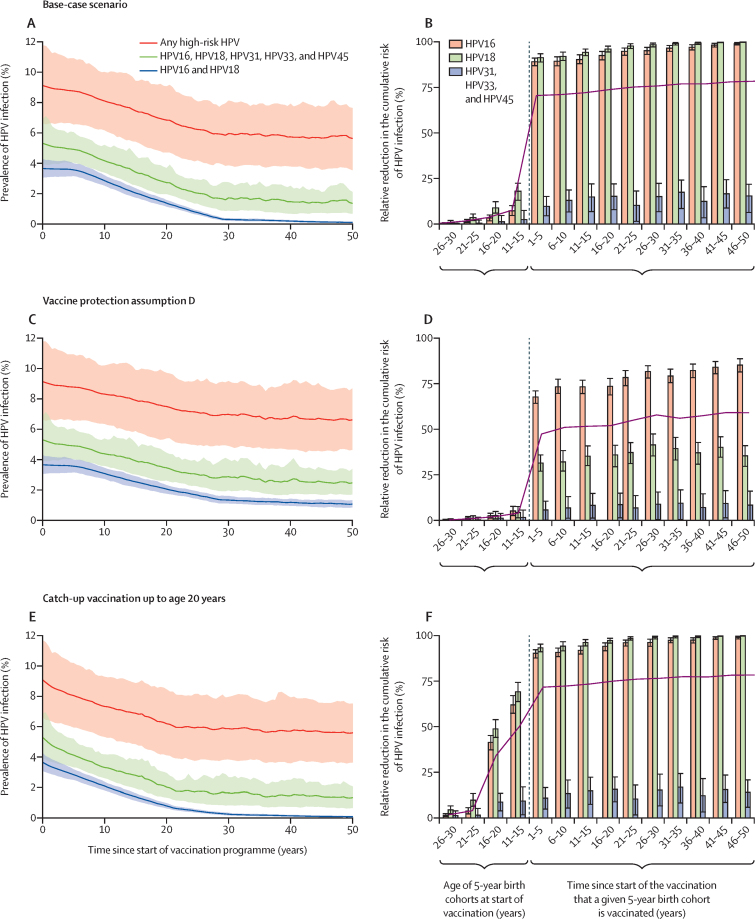
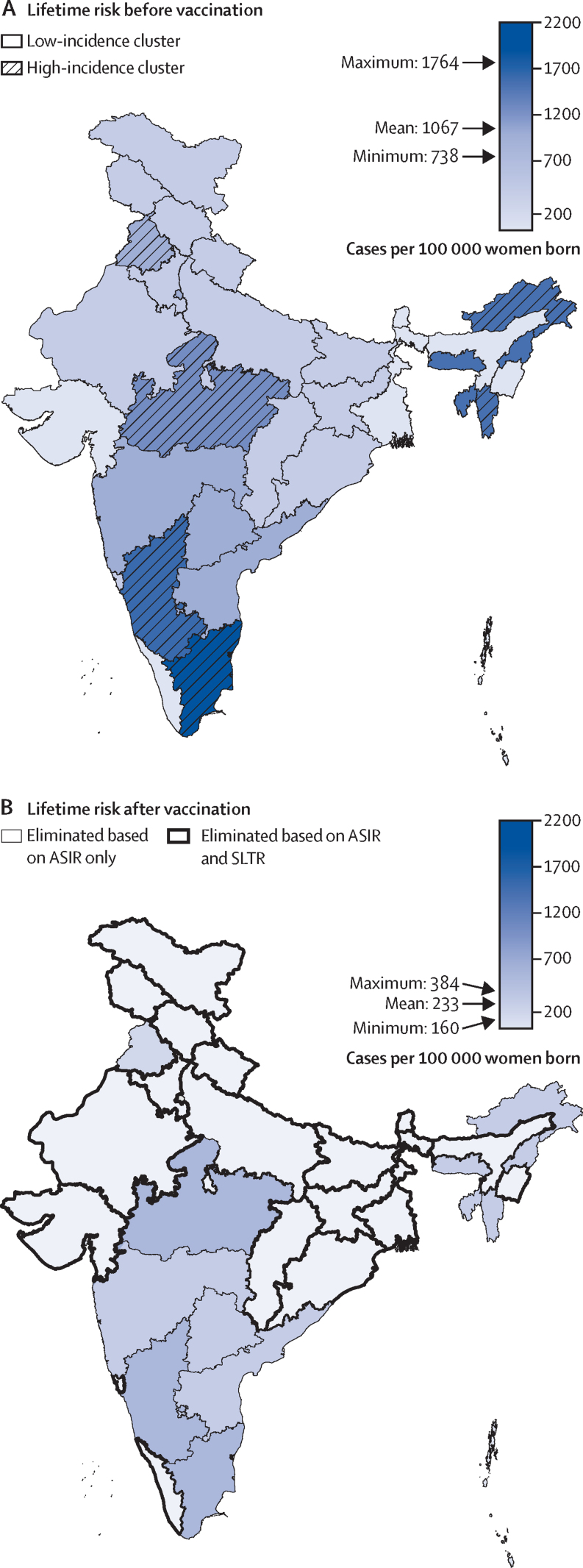
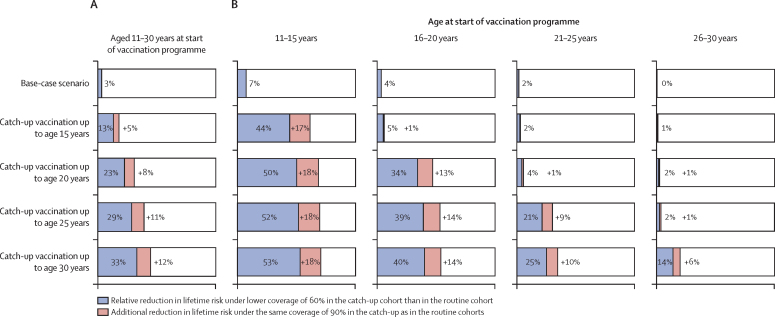
Findings: Assuming vaccination in girls aged 10 years, with 90% coverage, and life-long protection by two-dose or single-dose schedule, HPV vaccination could reduce the prevalence of HPV16 and HPV18 infection by 97% (80% UI 96-99) in 50 years, and the lifetime risk of cervical cancer by 71-78% from 1067 cases per 100 000 women born under a no vaccination scenario to 311 (80% UI 284-339) cases per 100 000 women born in the short term and 233 (219-252) cases per 100 000 women born in the long term in vaccinated cohorts. Under this scenario, we projected that the age-standardised incidence rate threshold for elimination could be met across India (range across Indian states: 1·6 cases [80% UI 1·5-1·7] to 4·0 cases [3·8-4·4] per 100 000 woman-years), while the complementary threshold based on standardised lifetime risk was attainable in 17 (68%) of 25 states, but not nationwide (range across Indian states: 207 cases [80% UI 194-223] to 477 cases [447-514] per 100 000 women born). Under the considered assumptions of waning vaccine protection, single-dose vaccination was projected to have a 21-100% higher per-dose efficiency than two-dose vaccination. Single-dose vaccination with catch-up for girls and women aged 11-20 years was more impactful than two-dose vaccination without catch-up, with reduction of 39-65% versus 38% in lifetime risk of cervical cancer across the ten catch-up birth cohorts and the first ten routine vaccination birth cohorts.
Interpretation: Our evidence-based projections suggest that scaling up cervical cancer prevention through single-dose HPV vaccination could substantially reduce cervical cancer burden in India.
Funding: The Bill & Melinda Gates Foundation.
© 2022 World Health Organization; licensee Elsevier. This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Conflict of interest statement
Declaration of interests JB has received support to his institution from IARC/WHO outside of the submitted work. All other authors declare no competing interests.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Lei J, Ploner A, Elfström KM, et al. HPV vaccination and the risk of invasive cervical cancer. N Engl J Med. 2020;383:1340–1348. - PubMed
-
- Falcaro M, Castañon A, Ndlela B, et al. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: a register-based observational study. Lancet. 2021;398:2084–2092. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
