

Aspirin for Primary Prevention of Cardiovascular Events in Relation to Lipoprotein(a) Genotypes
- PMID: 36175048
- PMCID: PMC10025998
- DOI: 10.1016/j.jacc.2022.07.027
Aspirin for Primary Prevention of Cardiovascular Events in Relation to Lipoprotein(a) Genotypes
Erratum in
-
Correction.J Am Coll Cardiol. 2022 Nov 15;80(20):1963. doi: 10.1016/j.jacc.2022.10.002. J Am Coll Cardiol. 2022. PMID: 36357094 No abstract available.
Abstract
Background: The role of aspirin in reducing lipoprotein(a)-mediated atherothrombotic events in primary prevention is not established.
Objectives: This study sought to assess whether low-dose aspirin benefits individuals with elevated plasma lipoprotein(a)-associated genotypes in the setting of primary prevention.
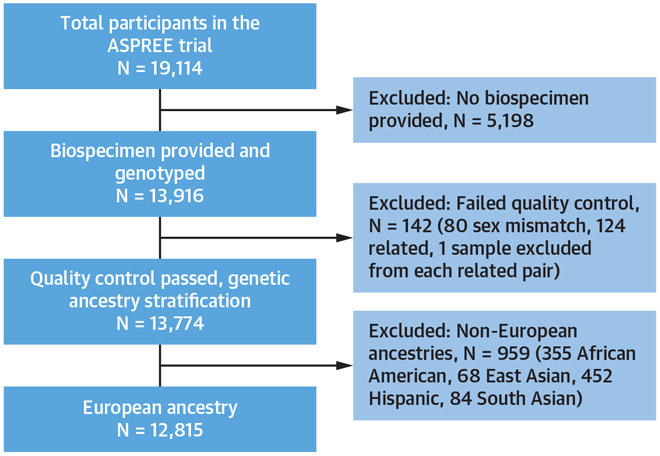
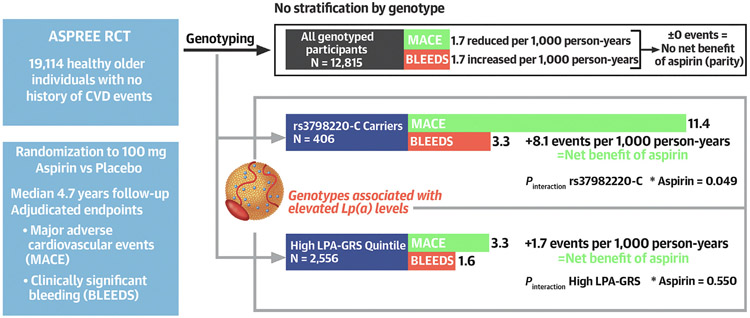
Methods: The study analyzed 12,815 genotyped individuals ≥70 years of age of European ancestry and without prior cardiovascular disease events enrolled in the ASPREE (ASPirin in Reducing Events in the Elderly) randomized controlled trial of 100 mg/d aspirin. We defined lipoprotein(a)-associated genotypes using rs3798220-C carrier status and quintiles of a lipoprotein(a) genomic risk score (LPA-GRS). We tested for interaction between genotypes and aspirin allocation in Cox proportional hazards models for incidence of major adverse cardiovascular events (MACE) and clinically significant bleeding. We also examined associations in the aspirin and placebo arms of the trial separately.
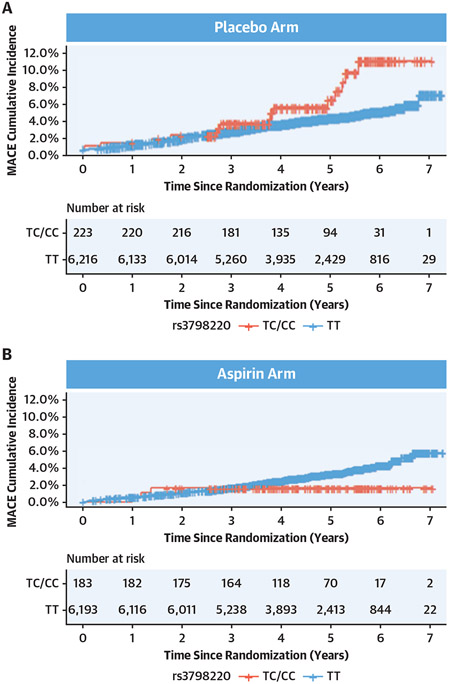
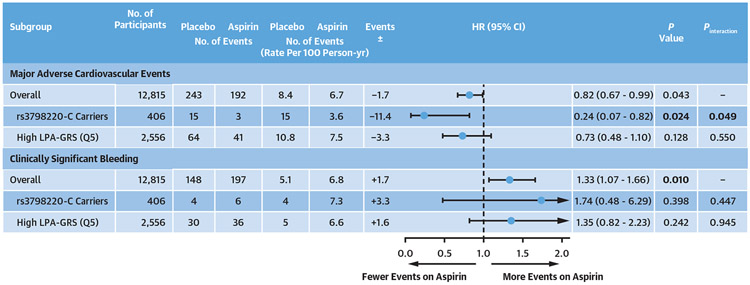
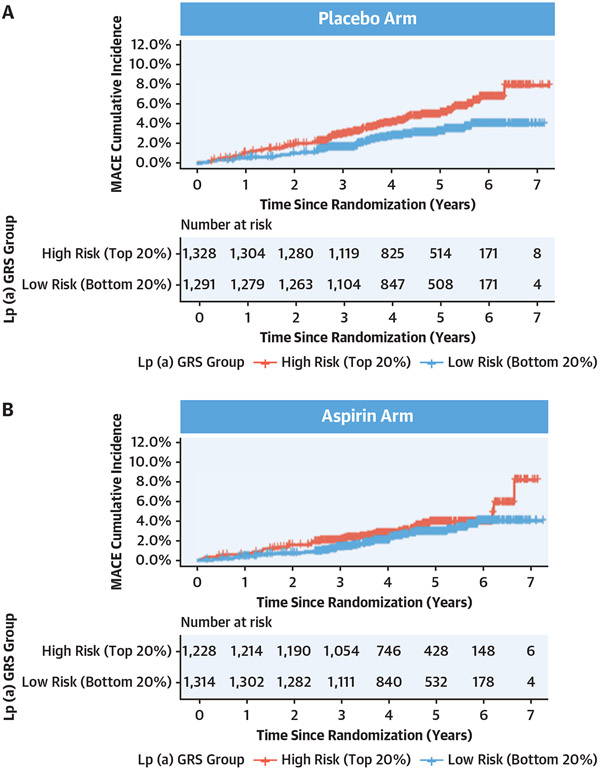
Results: During a median 4.7 years (IQR: 3.6-5.7 years) of follow-up, 435 MACE occurred, with an interaction observed between rs3798220-C and aspirin allocation (P = 0.049). rs3798220-C carrier status was associated with increased MACE risk in the placebo group (HR: 1.90; 95% CI: 1.11-3.24) but not in the aspirin group (HR: 0.54; 95% CI: 0.17-1.70). High LPA-GRS (vs low) was associated with increased MACE risk in the placebo group (HR: 1.70; 95% CI: 1.14-2.55), with risk attenuated in the aspirin group (HR: 1.41; 95% CI: 0.90-2.23), but the interaction was not statistically significant. In all participants, aspirin reduced MACE by 1.7 events per 1,000 person-years and increased clinically significant bleeding by 1.7 events per 1,000 person-years. However, in the rs3798220-C and high LPA-GRS subgroups, aspirin reduced MACE by 11.4 and 3.3 events per 1,000 person-years respectively, without significantly increased bleeding risk.
Conclusions: Aspirin may benefit older individuals with elevated lipoprotein(a) genotypes in primary prevention.
Keywords: aspirin; cardiovascular disease; genetics; lipoprotein(a); primary prevention.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The ASPREE Biobank is supported by a Flagship cluster grant (including the Commonwealth Scientific and Industrial Research Organisation, Monash University, Menzies Research Institute, Australian National University, University of Melbourne), grants U01AG029824 and U19AG062682 from the National Institute on Aging and the National Cancer Institute at the National Institutes of Health, by grants 334047 and 1127060 from the National Health and Medical Research Council of Australia, and Monash University and the Victorian Cancer Agency. Dr Lacaze is supported by a National Heart Foundation Future Leader Fellowship (102604). Dr McNeil is supported by a National Health and Medical Research Council Leadership Fellowship (IG1173690). Dr Bhatia is partially supported by National Institutes of Health grant 5T32HL079891, as part of the University of California San Diego Integrated Cardiovascular Epidemiology Fellowship. Dr Natarajan is supported by grants from the National Heart, Lung, and Blood Institute/National Institutes of Health (R01HL142711, R01HL127564). Bayer AG provided low-dose aspirin and placebo tablets for the clinical trial but had no other relationship with the work. Dr Riaz is a paid employee of Regeneron Genetics Center, a Subsidiary of Regeneron Pharmaceuticals Inc. Dr Natarajan has received investigator-initiated grants from Amgen, Apple, AstraZeneca, Boston Scientific, and Novartis; has received personal fees from Apple, AstraZeneca, Blackstone Life Sciences, Foresite Labs, Novartis, and Roche/Genentech; is a co-founder of TenSixteen Bio; is a shareholder of geneXwell and TenSixteen Bio; and has a spouse who is an employee of Vertex, all unrelated to the present work. Dr Nicholls has received research support from AstraZeneca, Amgen, Anthera, CSL Behring, Cerenis, Eli Lilly, Esperion, Resverlogix, Novartis, InfraReDx, and Sanofi-Regeneron; and has served as a consultant for Amgen, Akcea, AstraZeneca, Boehringer Ingelheim, CSL Behring, Eli Lilly, Esperion, Kowa, Merck, Takeda, Pfizer, Sanofi-Regeneron, and Novo Nordisk. Dr Tonkin has received research support from Bayer for materials in ASPREE; and has received honoraria for Advisory Board participation or lectures from Amgen, AstraZeneca, Boehringer Ingelheim, and Pfizer. Dr Tsimikas is a co-inventor and has received royalties from patents owned by the University of California-San Diego; is a co-founder of and has an equity interest in Oxitope, LLC and its affiliates (Kleanthi Diagnostics, LLC and Covicept Therapeutics, Inc); and has a dual appointment at the University of California San Diego and Ionis Pharmaceuticals; although these relationships have been identified for conflict-of-interest management based on the overall scope of the project, the research findings included in this particular publication may not necessarily relate to the interests of the previous companies; the terms of this arrangement have been reviewed and approved by the University of California San Diego in accordance with its conflict-of-interest policies. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Lp(a): Are Antithrombotic Therapies the Key to Event Reduction?J Am Coll Cardiol. 2022 Oct 4;80(14):1299-1301. doi: 10.1016/j.jacc.2022.08.722. J Am Coll Cardiol. 2022. PMID: 36175049 No abstract available.
References
-
- Tsimikas S, Karwatowska-Prokopczuk E, Gouni-Berthold I, et al. Lipoprotein(a) reduction in persons with cardiovascular disease. N Engl J Med. 2020;382:244–255. - PubMed
-
- Varvel S, McConnell JP, Tsimikas S. Prevalence of elevated Lp(a) mass levels and patient thresholds in 532 359 patients in the United States. Arterioscler Thromb Vasc Biol. 2016;36:2239–2245. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
