

A Standardized and Regionalized Network of Care for Cardiogenic Shock
- PMID: 36175063
- PMCID: PMC10404382
- DOI: 10.1016/j.jchf.2022.04.004
A Standardized and Regionalized Network of Care for Cardiogenic Shock
Abstract
Background: The benefits of standardized care for cardiogenic shock (CS) across regional care networks are poorly understood.
Objectives: The authors compared the management and outcomes of CS patients initially presenting to hub versus spoke hospitals within a regional care network.
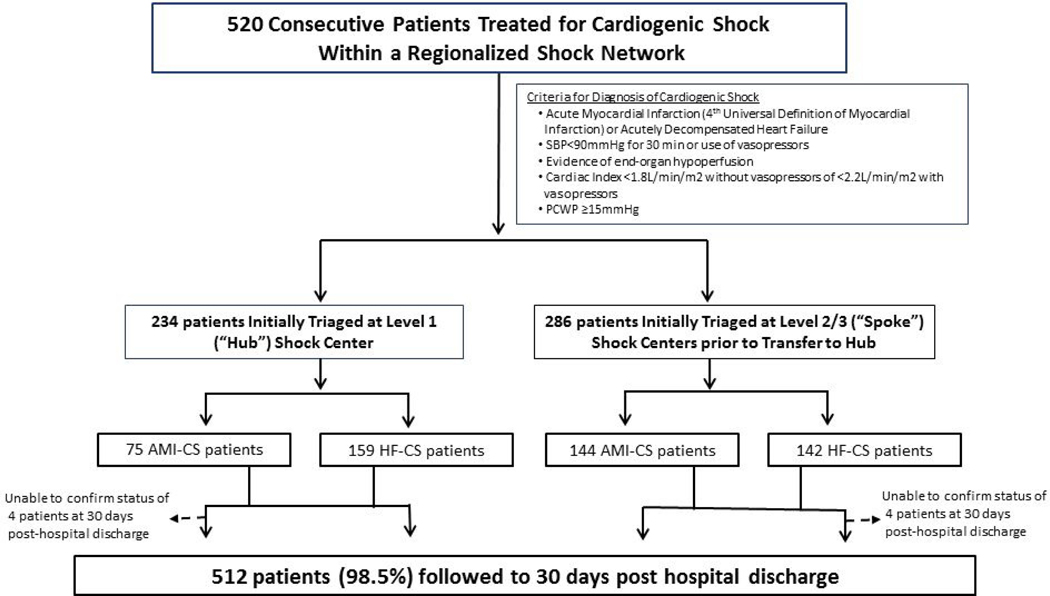
Methods: The authors stratified consecutive patients enrolled in their CS registry (January 2017 to December 2019) by presentation to a spoke versus the hub hospital. The primary endpoint was 30-day mortality. Secondary endpoints included bleeding, stroke, or major adverse cardiovascular and cerebrovascular events.
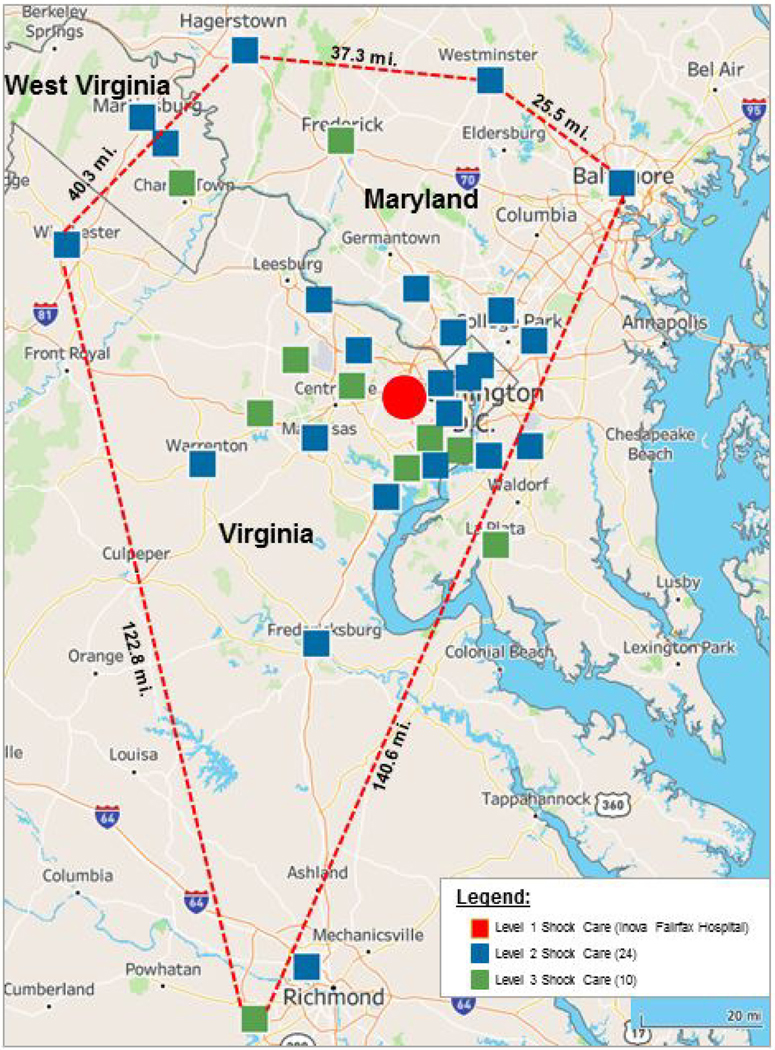
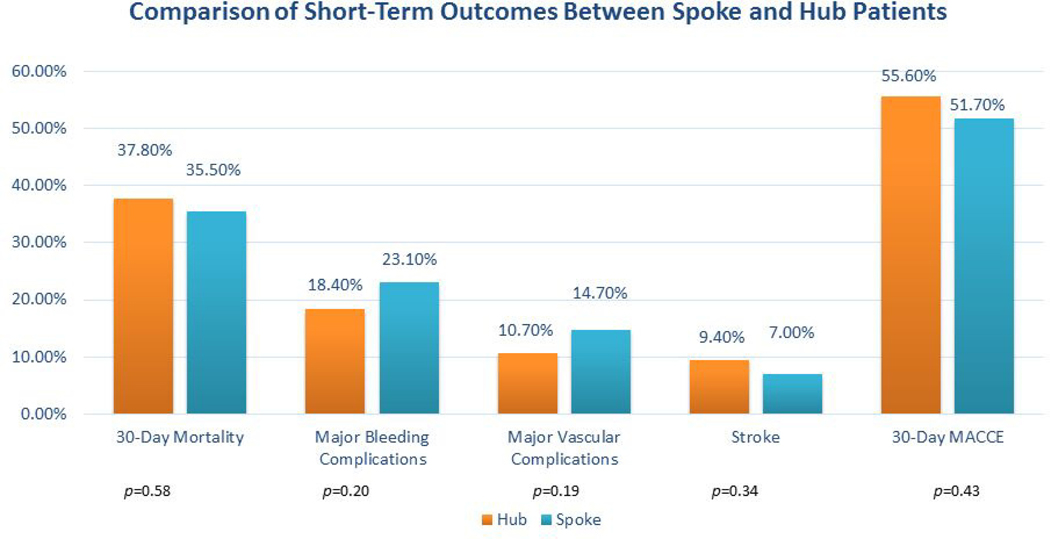
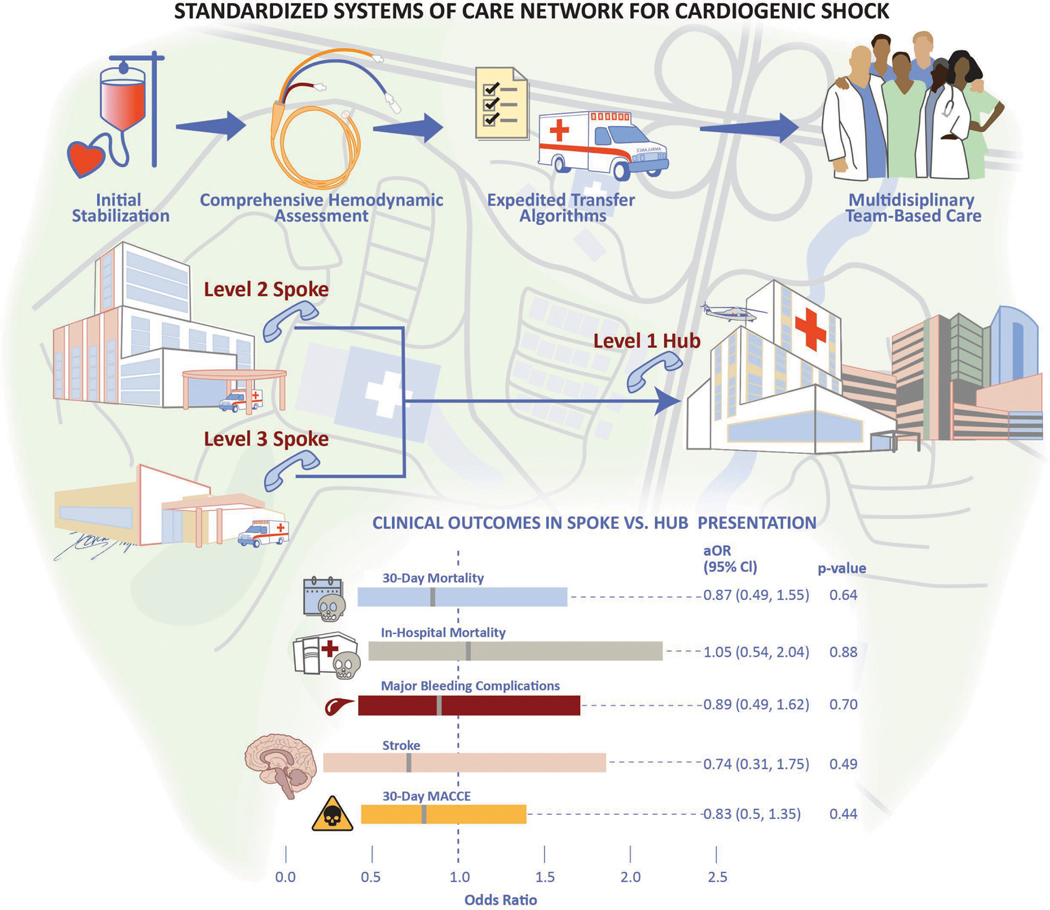
Results: Of 520 CS patients, 286 (55%) initially presented to 34 spoke hospitals. No difference in mean age (62 years vs 61 years; P = 0.38), sex (25% vs 32% women; P = 0.10), and race (54% vs 52% white; P = 0.82) between spoke and hub patients was noted. Spoke patients more often presented with acute myocardial infarction (50% vs 32%; P < 0.01), received vasopressors (74% vs 66%; P = 0.04), and intra-aortic balloon pumps (88% vs 37%; P < 0.01). Hub patients were more often supported with percutaneous ventricular assist devices (44% vs 11%; P < 0.01) and veno-arterial extracorporeal membrane oxygenation (13% vs 0%; P < 0.01). Initial presentation to a spoke was not associated with increased risk-adjusted 30-day mortality (adjusted OR: 0.87 [95% CI: 0.49-1.55]; P = 0.64), bleeding (adjusted OR: 0.89 [95% CI: 0.49-1.62]; P = 0.70), stroke (adjusted OR: 0.74 [95% CI: 0.31-1.75]; P = 0.49), or major adverse cardiovascular and cerebrovascular events (adjusted OR 0.83 [95% CI: 0.50-1.35]; P = 0.44).
Conclusions: Spoke and hub patients experienced similar short-term outcomes within a regionalized CS network. The optimal strategy to promote standardized care and improved outcomes across regional CS networks merits further investigation.
Keywords: cardiogenic shock; hub and spoke networks; systems of care.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Tehrani has served on the advisory board for Abbott; has received research grants from Boston Scientific and Inari Medical; and has served as a consultant for Boston Scientific. Dr Truesdell has served as a consultant for Abiomed. Dr Ibrahim has received honoraria from Medtronic. Dr Shah is supported by a National Institutes of Health K23 Career Development Award 1K23HL143179; has served as a consultant for Merck, Novartis, and Procyrion; and his institution has received grant support from Abbott, Roche, Merck and Bayer for unrelated research. Dr Batchelor has served as consultant for Boston Scientific, Abbott, Medtronic, and V-Wave. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
Association of Use of an Intravascular Microaxial Left Ventricular Assist Device vs Intra-aortic Balloon Pump With In-Hospital Mortality and Major Bleeding Among Patients With Acute Myocardial Infarction Complicated by Cardiogenic Shock.JAMA. 2020 Feb 25;323(8):734-745. doi: 10.1001/jama.2020.0254. JAMA. 2020. PMID: 32040163 Free PMC article.
-
Prospective Comparison of a Percutaneous Ventricular Assist Device and Venoarterial Extracorporeal Membrane Oxygenation for Patients With Cardiogenic Shock Following Acute Myocardial Infarction.J Am Heart Assoc. 2019 May 7;8(9):e012171. doi: 10.1161/JAHA.119.012171. J Am Heart Assoc. 2019. PMID: 31041870 Free PMC article.
-
Informing Management of Patients Developing Cardiogenic Shock at a Spoke and Being Transferred to a Hub.J Am Heart Assoc. 2025 Feb 18;14(4):e035464. doi: 10.1161/JAHA.124.035464. Epub 2025 Feb 14. J Am Heart Assoc. 2025. PMID: 39950322 Free PMC article.
-
Mechanical assist devices for acute cardiogenic shock.Cochrane Database Syst Rev. 2020 Jun 4;6(6):CD013002. doi: 10.1002/14651858.CD013002.pub2. Cochrane Database Syst Rev. 2020. PMID: 32496607 Free PMC article.
-
Comparative safety of percutaneous ventricular assist device and intra-aortic balloon pump in acute myocardial infarction-induced cardiogenic shock.Open Heart. 2021 Jun;8(1):e001662. doi: 10.1136/openhrt-2021-001662. Open Heart. 2021. PMID: 34127531 Free PMC article. Review.
Cited by
-
Position Statement on Vascular Access Safety for Percutaneous Devices in AMI Complicated by Cardiogenic Shock.JACC Cardiovasc Interv. 2022 Oct 24;15(20):2003-2019. doi: 10.1016/j.jcin.2022.08.041. JACC Cardiovasc Interv. 2022. PMID: 36265932 Free PMC article. Review.
-
The Price We Pay for Progression in Shock Care: Economic Burden, Accessibility, and Adoption of Shock-Teams and Mechanical Circulatory Support Devices.Curr Cardiol Rep. 2024 Oct;26(10):1123-1134. doi: 10.1007/s11886-024-02108-4. Epub 2024 Sep 26. Curr Cardiol Rep. 2024. PMID: 39325244 Review.
-
From Spoke to Hub: The "Golden Hours" in Cardiogenic Shock.J Am Heart Assoc. 2025 Feb 18;14(4):e039100. doi: 10.1161/JAHA.124.039100. Epub 2025 Feb 14. J Am Heart Assoc. 2025. PMID: 39950350 Free PMC article. No abstract available.
-
Clinical Characteristics and Outcomes of Patients Suffering Acute Decompensated Heart Failure Complicated by Cardiogenic Shock.Circ Heart Fail. 2024 Sep;17(9):e011358. doi: 10.1161/CIRCHEARTFAILURE.123.011358. Epub 2024 Aug 29. Circ Heart Fail. 2024. PMID: 39206544
-
Defining levels of care in cardiogenic shock.Front Cardiovasc Med. 2023 Oct 31;10:1206570. doi: 10.3389/fcvm.2023.1206570. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 38028504 Free PMC article.
References
-
- Vallabhajosyula S, Dunlay SM, Barsness GW, Rihal CS, Holmes DR Jr., Prasad A. Hospital-Level Disparities in the Outcomes of Acute Myocardial Infarction With Cardiogenic Shock. Am J Cardiol 2019;124:491–498. - PubMed
-
- Wayangankar SA, Bangalore S, McCoy LA et al. Temporal Trends and Outcomes of Patients Undergoing Percutaneous Coronary Interventions for Cardiogenic Shock in the Setting of Acute Myocardial Infarction: A Report From the CathPCI Registry. JACC Cardiovasc Interv 2016;9:341–351. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
