

Frequency of New or Enlarging Lesions on MRI Outside of Clinical Attacks in Patients With MOG-Antibody-Associated Disease
- PMID: 36175150
- PMCID: PMC9651461
- DOI: 10.1212/WNL.0000000000201263
Frequency of New or Enlarging Lesions on MRI Outside of Clinical Attacks in Patients With MOG-Antibody-Associated Disease
Abstract
Background and objective: To determine the frequency of new or enlarging T2-hyperintense or enhancing lesions outside of clinical attacks in myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) vs multiple sclerosis (MS) and aquaporin-4 antibody positive neuromyelitis optica spectrum disorder (AQP4+NMOSD).
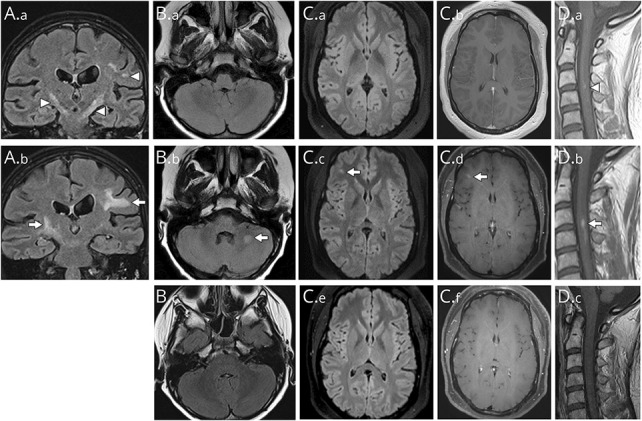
Methods: We retrospectively included Mayo Clinic patients with MOGAD with: (1) MOG-Immunoglobulin-G positivity by live cell-based assay, (2) fulfilling proposed MOGAD diagnostic criteria, and (3) baseline and follow-up paired MRIs without interval attacks. A neurologist and neuroradiologist reviewed MRIs (T2-fluid attenuated inversion recovery brain, T2 spine, and T1-postgadolinium brain and spine) to identify new or enlarging lesions. A MOGAD subset was then compared to patients with MS and AQP4+NMOSD, based on broadly similar interscan intervals.
Results: We included 105 patients with MOGAD (median age, 31 years [range, 2-80]; 60% female) with 373 paired MRIs. In total, 10/105 (9.5%) patients and 13/373 (3%) scans had one or more new T2 lesions (brain, 12/213 [6%]; spine, 1/160 [0.6%]); and 8/367 (2%) had enhancing lesions. New brain lesions were less in MOGAD (1/25 [4%]) than MS (14/26 [54%], p < 0.0001) but did not differ from AQP4+NMOSD (1/13 [8%], p = 1.0) in subgroup analysis. New spinal lesions were rare across groups (0%-4%).
Discussion: New or enlarging MRI lesions rarely develop outside of clinical attacks in MOGAD differing from MS. Surveillance MRIs in MOGAD have limited utility with implications for clinical practice and trial design.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Marignier R, Hacohen Y, Cobo-Calvo A, et al. . Myelin-oligodendrocyte glycoprotein antibody-associated disease. Lancet Neurol. 2021;20(9):762-772. - PubMed
-
- Wattjes MP, Ciccarelli O, Reich DS, et al. . 2021 MAGNIMS-CMSC-NAIMS consensus recommendations on the use of MRI in patients with multiple sclerosis. Lancet Neurol. 2021;20(8):653-670. - PubMed
-
- Lee MY, Yong KP, Hyun JW, Kim SH, Lee SH, Kim HJ. Incidence of interattack asymptomatic brain lesions in NMO spectrum disorder. Neurology. 2020;95(23):e3124-e3128. - PubMed
-
- Fadda G, Banwell B, Waters P, et al. . Silent new brain MRI lesions in children with MOG-antibody associated disease. Ann Neurol. 2021;89(2):408-413. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical