

Item response theory and differential test functioning analysis of the HBSC-Symptom-Checklist across 46 countries
- PMID: 36175865
- PMCID: PMC9520881
- DOI: 10.1186/s12874-022-01698-3
Item response theory and differential test functioning analysis of the HBSC-Symptom-Checklist across 46 countries
Abstract
Background: The Symptom Checklist (SCL) developed by the Health Behaviour in School-aged Children (HBSC) study is a non-clinical measure of psychosomatic complaints (e.g., headache and feeling low) that has been used in numerous studies. Several studies have investigated the psychometric characteristics of this scale; however, some psychometric properties remain unclear, among them especially a) dimensionality, b) adequacy of the Graded Response Model (GRM), and c) measurement invariance across countries.
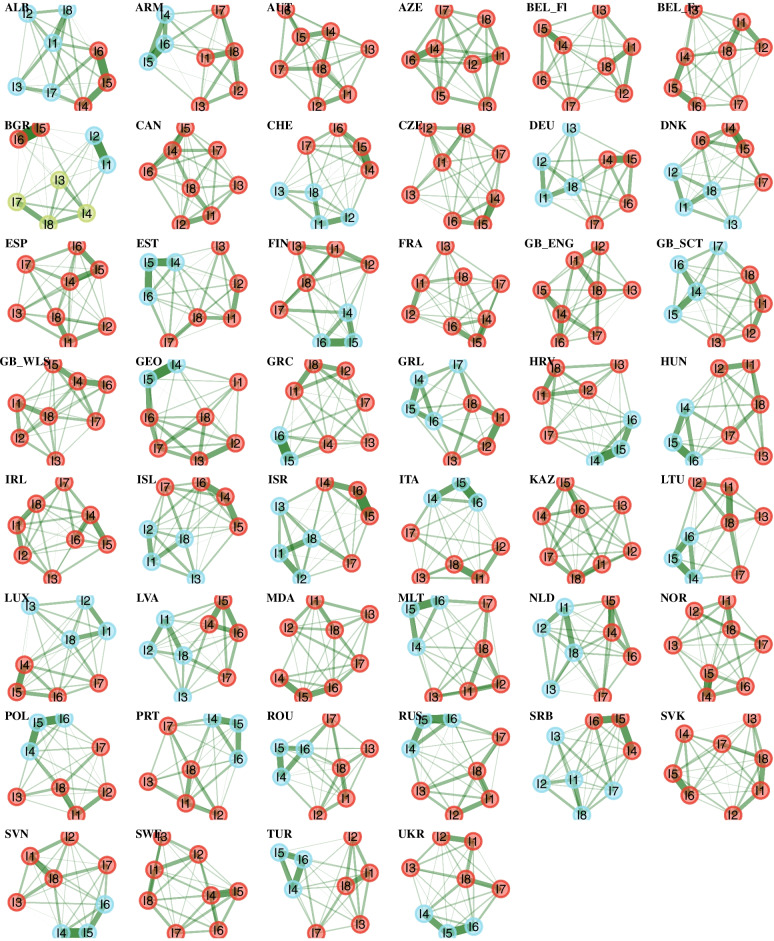
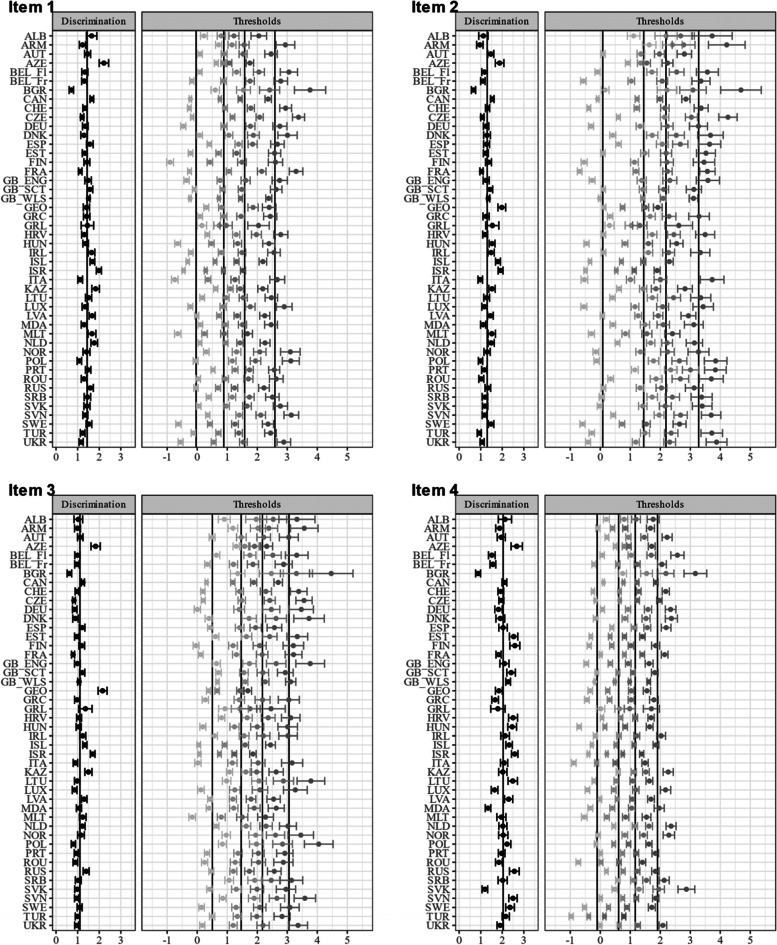
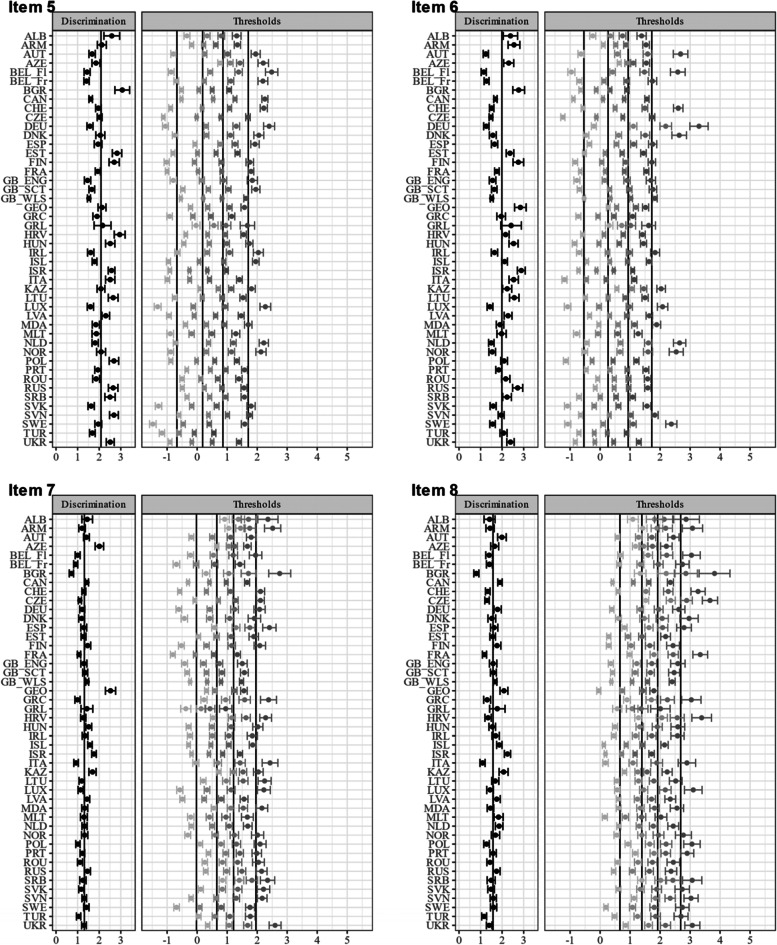
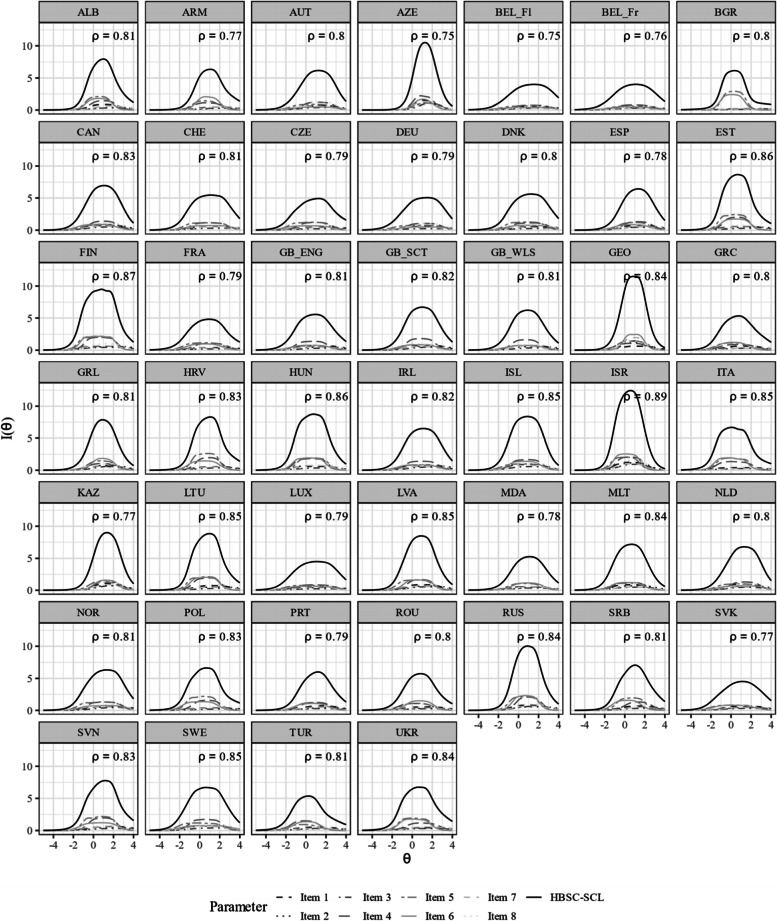
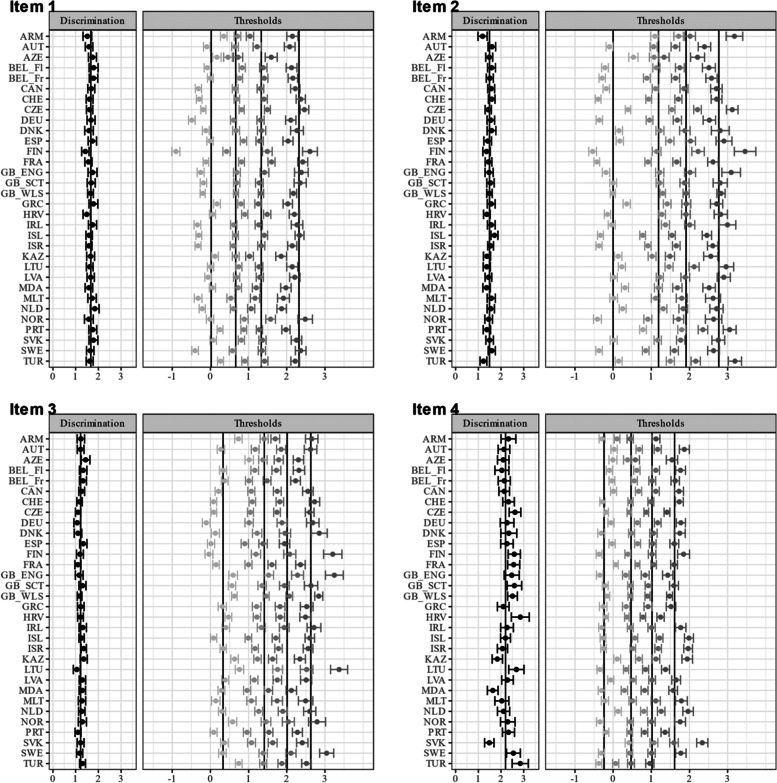
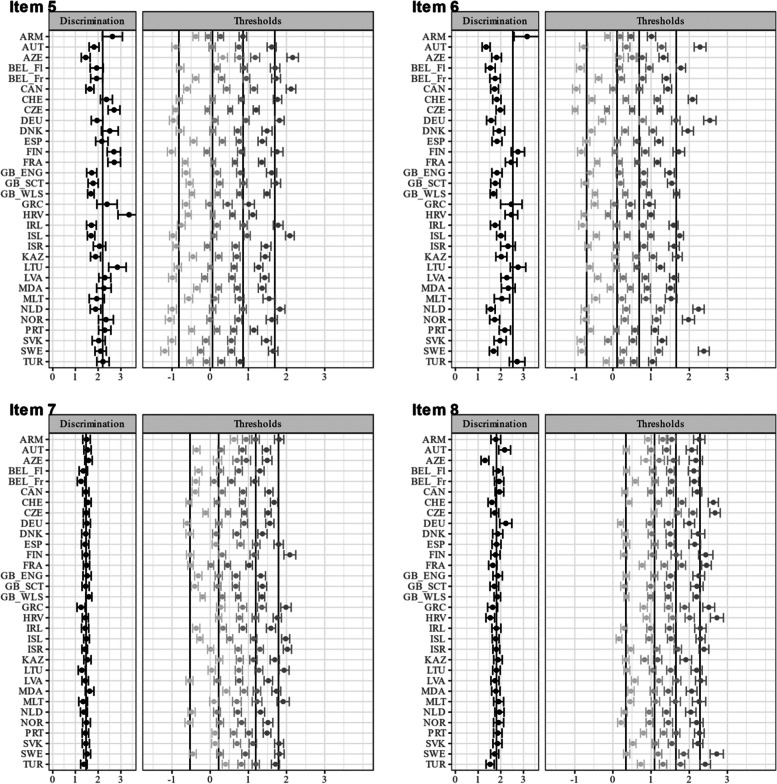
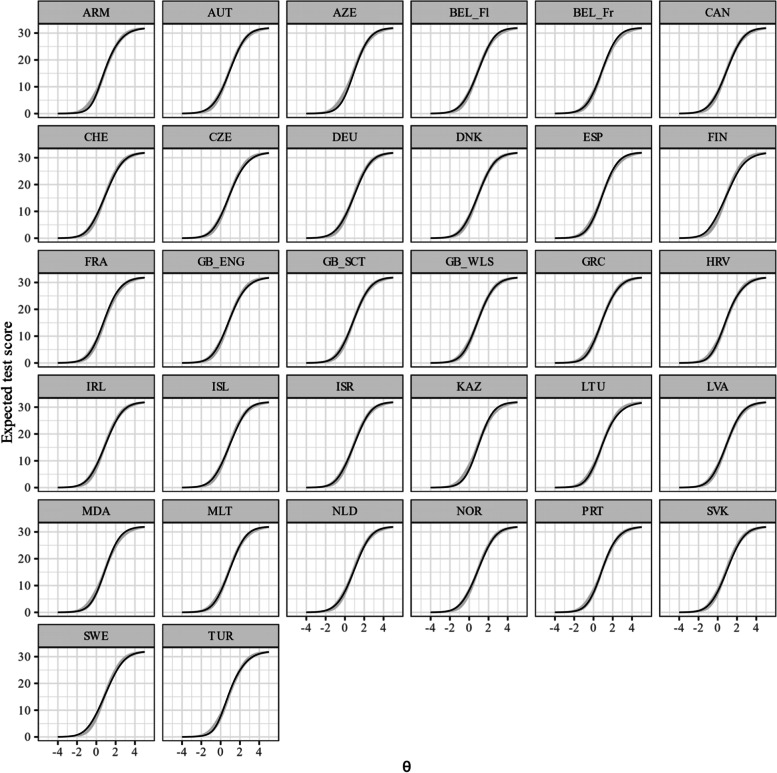
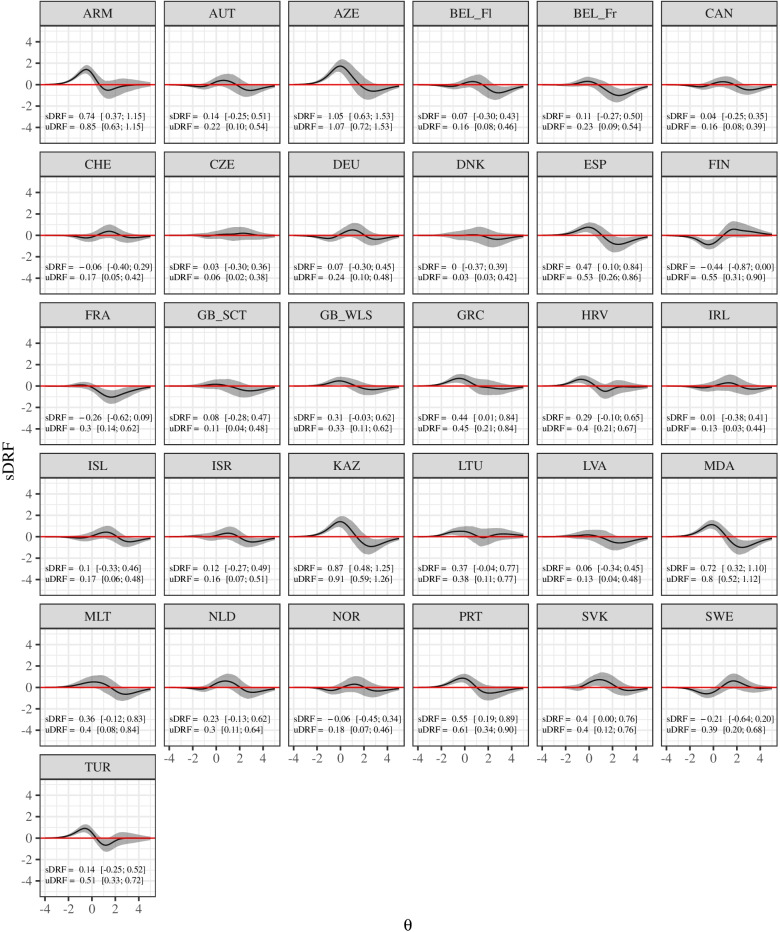
Methods: Data from 229,906 adolescents aged 11, 13 and 15 from 46 countries that participated in the 2018 HBSC survey were analyzed. Adolescents were selected using representative sampling and surveyed by questionnaire in the classroom. Dimensionality was investigated using exploratory graph analysis. In addition, we investigated whether the GRM provided an adequate description of the data. Reliability over the latent variable continuum and differential test functioning across countries were also examined.
Results: Exploratory graph analyses showed that SCL can be considered as one-dimensional in 16 countries. However, a comparison of the unidimensional with a post-hoc bifactor GRM showed that deviation from a hypothesized one-dimensional structure was negligible in most countries. Multigroup invariance analyses supported configural and metric invariance, but not scalar invariance across 32 countries. Alignment analysis showed non-invariance especially for the items irritability, feeling nervous/bad temper and feeling low.
Conclusion: HBSC-SCL appears to represent a consistent and reliable unidimensional instrument across most countries. This bodes well for population health analyses that rely on this scale as an early indicator of mental health status.
Keywords: Adolescents; Cross-national; Differential item functioning; HBSC symptom checklist; Health behaviour in school-aged children; Measurement invariance; Psychosomatic health complaints; Self-reported health complaints; Subjective health complaints.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
