

Epidemiology, treatment patterns, clinical outcomes, and disease burden among patients with immune-mediated thrombotic thrombocytopenic purpura in the United States
- PMID: 36176310
- PMCID: PMC9481884
- DOI: 10.1002/rth2.12802
Epidemiology, treatment patterns, clinical outcomes, and disease burden among patients with immune-mediated thrombotic thrombocytopenic purpura in the United States
Abstract
Background: Immune-mediated thrombotic thrombocytopenic purpura (iTTP) is a life-threatening thrombotic microangiopathy. Due to its rarity, epidemiology and real-world outcomes data are scarce.
Objectives: The aim was to assess epidemiology, treatment patterns, clinical outcomes, and disease burden in patients with iTTP in the United States.
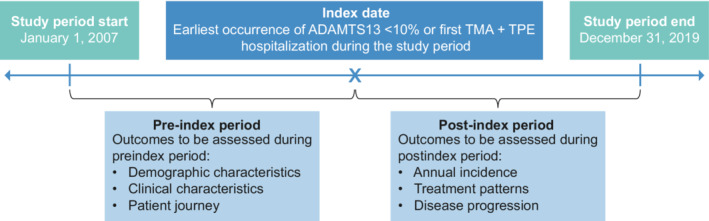
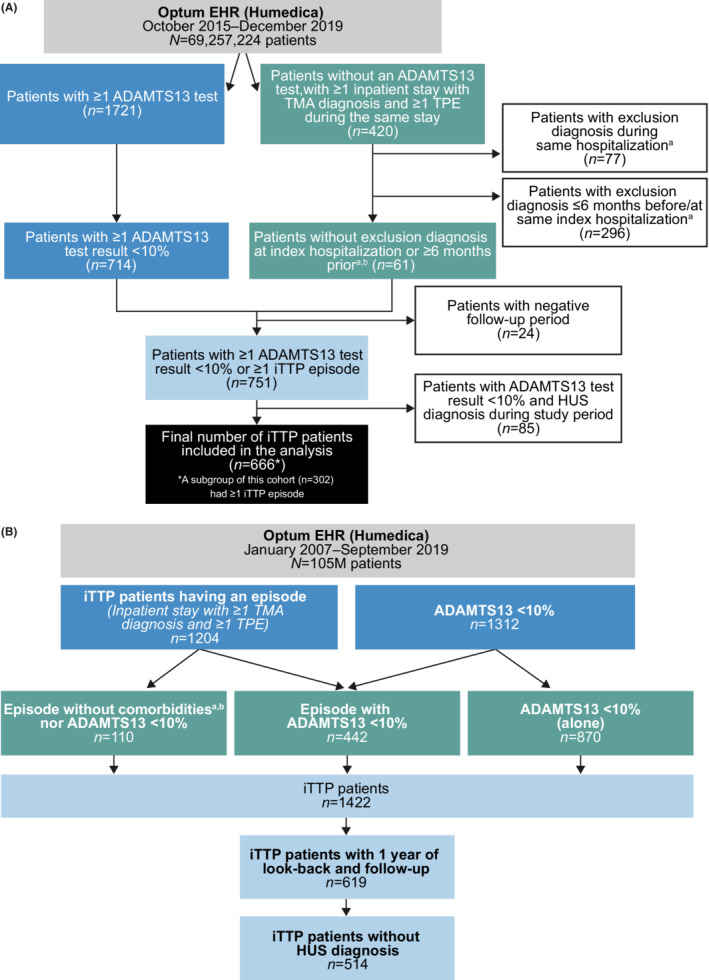
Methods: This longitudinal, retrospective observational study of the Optum-Humedica database included patients with an iTTP diagnosis (≥1 documented ADAMTS13 activity less than 10% or one or more iTTP episodes) from January 2007 to December 2019.
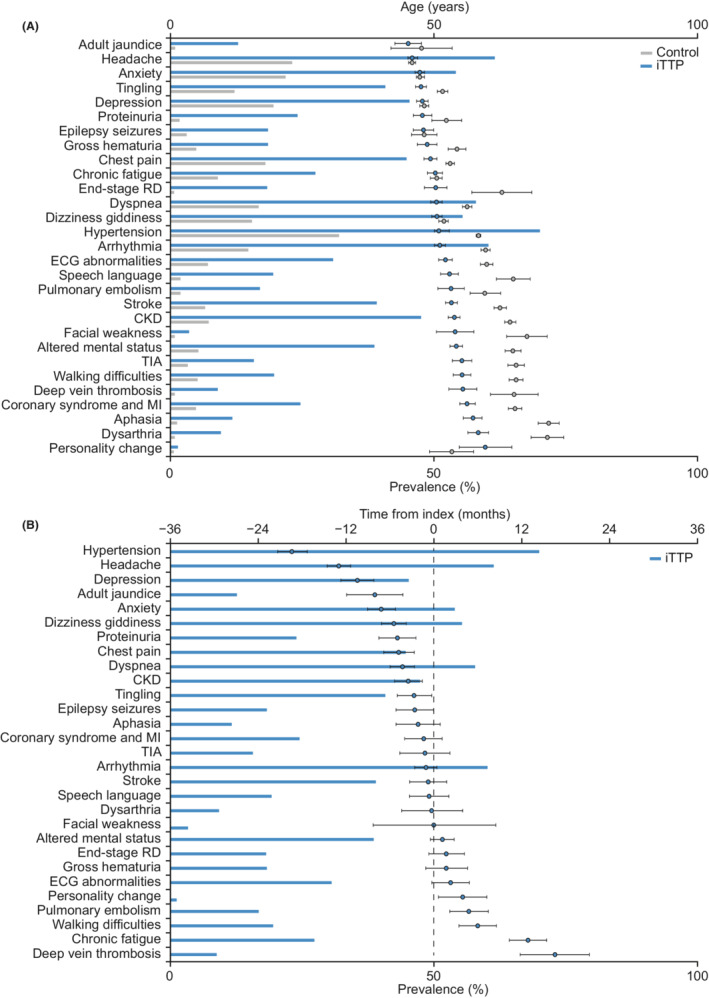
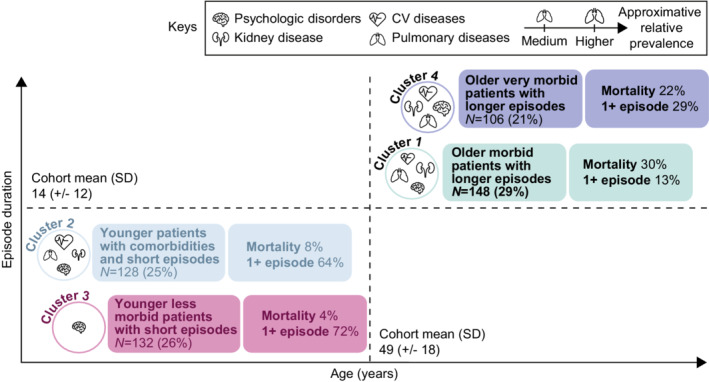
Results: Of 666 patients with an iTTP diagnosis between October 2015 and December 2019, 302 (45%) had one or more iTTP episodes. The pooled annual incidence of documented iTTP during this period was 3.43/million, and the annual incidence of one or more iTTP episodes was 1.81/million. Patients with one or more iTTP episodes received a median of six therapeutic plasma exchange (TPE) sessions per episode; 86% received corticosteroids, and 59% received rituximab. Exacerbations occurred in 17% (52/302) and relapse in 11% (34/302); 34% (103/302) had one or more thromboembolic events. Mortality rates during the study period were 25% (167/666) among all patients with iTTP diagnosis, and 14% (41/302) among patients with one or more iTTP episodes. In the assessment of disease burden (January 2007 to September 2019), patients in the iTTP cohort (n = 514) presented with a mean of 14 comorbidities, compared with 3 in a matched non-iTTP cohort (n = 2570). In a cluster analysis, duration of iTTP episode and mortality rate were greater in older versus younger patients.
Conclusions: Despite treatment with TPE and immunosuppressants, patients with iTTP have high risk of morbidity and mortality, demonstrating the need for more effective therapies.
Keywords: blood platelets; epidemiology; morbidity; thrombotic microangiopathies; thrombotic thrombocytopenic purpura.
© 2022 The Authors. Research and Practice in Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis (ISTH).
Figures
Similar articles
-
A Descriptive 5-Year Analysis of the Demographics and Therapies for Patients With Immune Thrombotic Thrombocytopenic Purpura in the USA: A Multicenter Study of 390 Disease Episodes From 2017 to 2021.J Clin Apher. 2025 Apr;40(2):e70017. doi: 10.1002/jca.70017. J Clin Apher. 2025. PMID: 40145682 Free PMC article.
-
Incidence, diagnosis, and outcome of immune-mediated thrombotic thrombocytopenic purpura: A nationwide survey by the Spanish registry of thrombotic thrombocytopenic purpura.J Clin Apher. 2021 Aug;36(4):563-573. doi: 10.1002/jca.21894. Epub 2021 Mar 29. J Clin Apher. 2021. PMID: 33780553
-
Taking Empiricism out of Immune Thrombotic Thrombocytopenic Purpura: Current and Future Treatment Strategies.Transfus Med Rev. 2019 Oct;33(4):248-255. doi: 10.1016/j.tmrv.2019.06.005. Epub 2019 Aug 15. Transfus Med Rev. 2019. PMID: 31645275 Review.
-
Management of immune thrombotic thrombocytopenic purpura with caplacizumab: a Canadian, single-centre, real-world experience.Platelets. 2023 Dec;34(1):2157807. doi: 10.1080/09537104.2022.2157807. Platelets. 2023. PMID: 36636834
-
A Systematic Review of the Epidemiology and Disease Burden of Congenital and Immune-Mediated Thrombotic Thrombocytopenic Purpura.J Blood Med. 2024 Aug 14;15:363-386. doi: 10.2147/JBM.S464365. eCollection 2024. J Blood Med. 2024. PMID: 39161536 Free PMC article. Review.
Cited by
-
Thrombotic Thrombocytopenic Purpura and Evans Syndrome: Validating and Exploring 20 Years of Routine Hospital Care.J Blood Med. 2025 Jun 7;16:279-292. doi: 10.2147/JBM.S513578. eCollection 2025. J Blood Med. 2025. PMID: 40502537 Free PMC article.
-
Acquired thrombotic thrombocytopenic purpura in a patient with plasmodium vivax malaria: A case report.Rev Soc Bras Med Trop. 2024 Sep 2;57:e008072024. doi: 10.1590/0037-8682-0014-2024. eCollection 2024. Rev Soc Bras Med Trop. 2024. PMID: 39230164 Free PMC article.
-
Cost-effectiveness of caplacizumab in immune thrombotic thrombocytopenic purpura in the United States.J Manag Care Spec Pharm. 2025 Mar;31(3):277-288. doi: 10.18553/jmcp.2025.31.3.277. J Manag Care Spec Pharm. 2025. PMID: 40021467 Free PMC article.
-
COVID-Induced Thrombotic Thrombocytopenic Purpura: A Case Report and Treatment-Focused Review.Cureus. 2024 Mar 30;16(3):e57252. doi: 10.7759/cureus.57252. eCollection 2024 Mar. Cureus. 2024. PMID: 38686279 Free PMC article.
-
A Descriptive 5-Year Analysis of the Demographics and Therapies for Patients With Immune Thrombotic Thrombocytopenic Purpura in the USA: A Multicenter Study of 390 Disease Episodes From 2017 to 2021.J Clin Apher. 2025 Apr;40(2):e70017. doi: 10.1002/jca.70017. J Clin Apher. 2025. PMID: 40145682 Free PMC article.
References
-
- Joly BS, Coppo P, Veyradier A. An update on pathogenesis and diagnosis of thrombotic thrombocytopenic purpura. Expert Rev Hematol. 2019;12(6):383‐395. - PubMed
-
- Kremer Hovinga JA, Coppo P, Lammle B, Moake JL, Miyata T, Vanhoorelbeke K. Thrombotic thrombocytopenic purpura. Nat Rev Dis Primers. 2017;3:17020. - PubMed
-
- Mariotte E, Azoulay E, Galicier L, et al. Epidemiology and pathophysiology of adulthood‐onset thrombotic microangiopathy with severe ADAMTS13 deficiency (thrombotic thrombocytopenic purpura): a cross‐sectional analysis of the French national registry for thrombotic microangiopathy. Lancet Haematol. 2016;3(5):e237‐e245. - PubMed
-
- George JN. How I treat patients with thrombotic thrombocytopenic purpura: 2010. Blood. 2010;116(20):4060‐4069. - PubMed
LinkOut - more resources
Full Text Sources
