

De-risking clinical trial failure through mechanistic simulation
- PMID: 36176591
- PMCID: PMC9514113
- DOI: 10.1093/immadv/ltac017
De-risking clinical trial failure through mechanistic simulation
Abstract
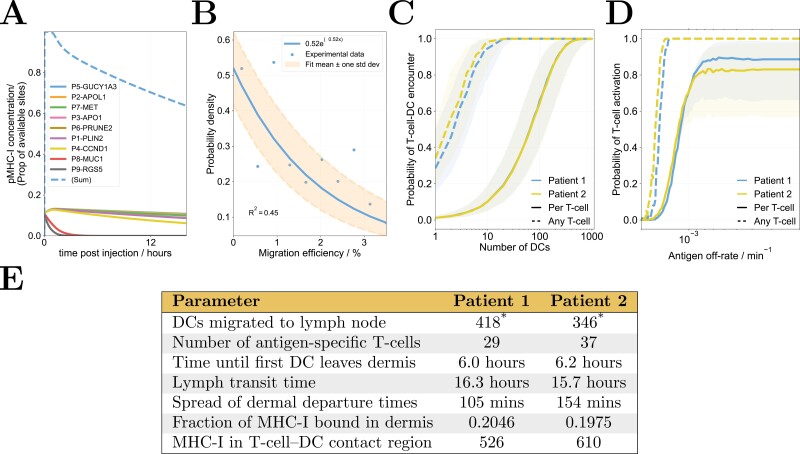
Drug development typically comprises a combination of pre-clinical experimentation, clinical trials, and statistical data-driven analyses. Therapeutic failure in late-stage clinical development costs the pharmaceutical industry billions of USD per year. Clinical trial simulation represents a key derisking strategy and combining them with mechanistic models allows one to test hypotheses for mechanisms of failure and to improve trial designs. This is illustrated with a T-cell activation model, used to simulate the clinical trials of IMA901, a short-peptide cancer vaccine. Simulation results were consistent with observed outcomes and predicted that responses are limited by peptide off-rates, peptide competition for dendritic cell (DC) binding, and DC migration times. These insights were used to hypothesise alternate trial designs predicted to improve efficacy outcomes. This framework illustrates how mechanistic models can complement clinical, experimental, and data-driven studies to understand, test, and improve trial designs, and how results may differ between humans and mice.
Keywords: late-phase trial; mathematical modelling; oncology; peptide; vaccines.
© The Author(s) 2022. Published by Oxford University Press on behalf of the British Society for Immunology.
Figures





References
-
- Trends, Charts, and Maps - ClinicalTrials.gov , Mar 2022. https://clinicaltrials.gov/ct2/resources/trends (8 March 2022, date last accessed).
Grants and funding
LinkOut - more resources
Full Text Sources