

A patient-driven clinicogenomic partnership for metastatic prostate cancer
- PMID: 36177448
- PMCID: PMC9518748
- DOI: 10.1016/j.xgen.2022.100169
A patient-driven clinicogenomic partnership for metastatic prostate cancer
Abstract
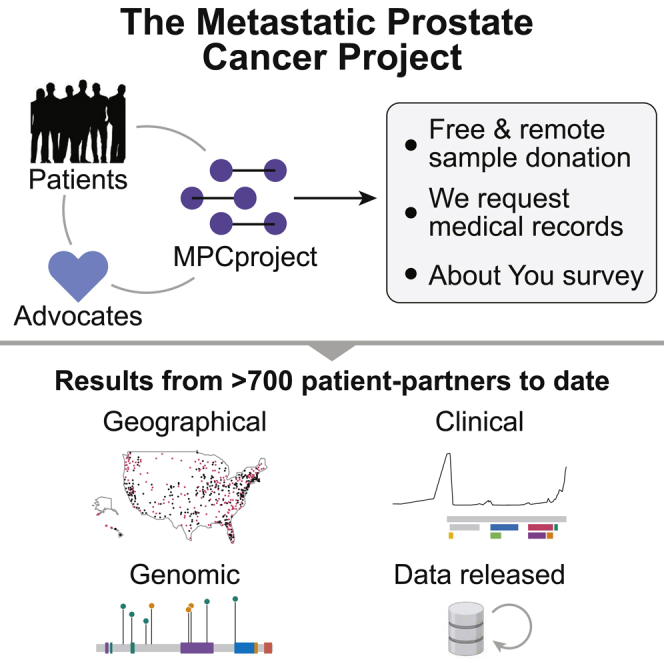
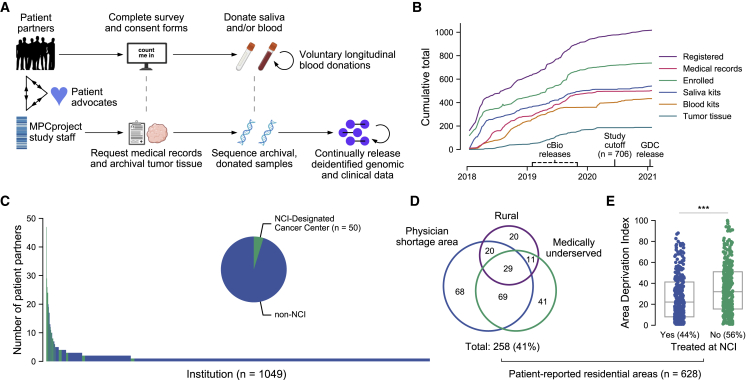
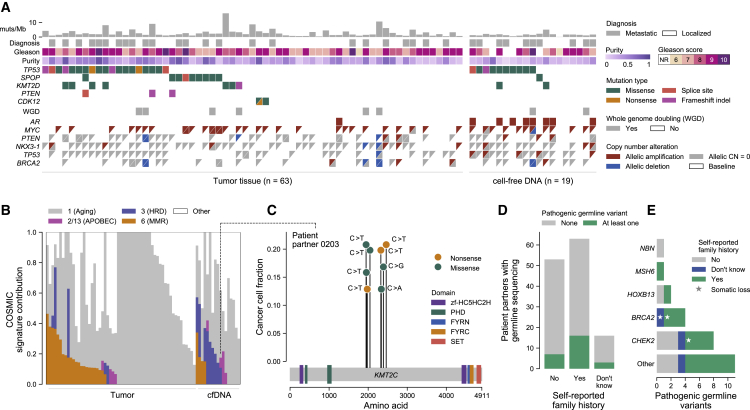
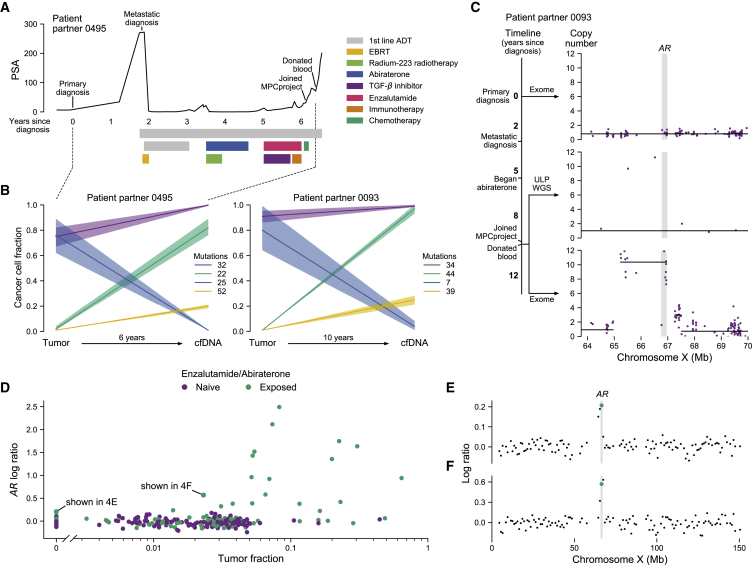
Molecular profiling studies have enabled discoveries for metastatic prostate cancer (MPC) but have predominantly occurred in academic medical institutions and involved non-representative patient populations. We established the Metastatic Prostate Cancer Project (MPCproject, mpcproject.org), a patient-partnered initiative to involve patients with MPC living anywhere in the US and Canada in molecular research. Here, we present results from our partnership with the first 706 MPCproject participants. While 41% of patient partners live in rural, physician-shortage, or medically underserved areas, the MPCproject has not yet achieved racial diversity, a disparity that demands new initiatives detailed herein. Among molecular data from 333 patient partners (572 samples), exome sequencing of 63 tumor and 19 cell-free DNA (cfDNA) samples recapitulated known findings in MPC, while inexpensive ultra-low-coverage sequencing of 318 cfDNA samples revealed clinically relevant AR amplifications. This study illustrates the power of a growing, longitudinal partnership with patients to generate a more representative understanding of MPC.
Conflict of interest statement
DECLARATION OF INTERESTS M.X.H. has been a consultant to Amplify Medicines and Ikena Oncology and is a current employee of Genentech/Roche. E.S.L. is currently in the process of divesting any relevant holdings. N.W. reports advisory relationships and consulting with Eli Lilly and Co.; advising and stockholding interest in Relay Therapeutics; and grant support from Puma Biotechnology. E.M.V.A. reports advisory relationships and consulting with Tango Therapeutics, Genome Medical, Invitae, Illumina, Enara Bio, Mani-fold Bio, and Janssen; research support from Novartis and BMS; equity in Tango Therapeutics, Genome Medical, Syapse, Mani-fold Bio, and Enara Bio; and travel reimbursement from Roche and Genentech, outside the submitted work.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
