

Correlation between endothelial dysfunction and occurrence of no-reflow in patients undergoing post-thrombolysis early invasive percutaneous intervention for ST-elevation myocardial infarction
- PMID: 36178560
- PMCID: PMC9525526
- DOI: 10.1186/s43044-022-00309-2
Correlation between endothelial dysfunction and occurrence of no-reflow in patients undergoing post-thrombolysis early invasive percutaneous intervention for ST-elevation myocardial infarction
Abstract
Background: Endothelial dysfunction and no-reflow share microcirculatory obstruction as a common pathophysiological mechanism. This study evaluated the relationship between systemic peripheral endothelial dysfunction assessed by flow-mediated dilatation (FMD) of the brachial artery and no-reflow in patients with ST-segment elevation myocardial infarction (STEMI) who received successful fibrinolysis.
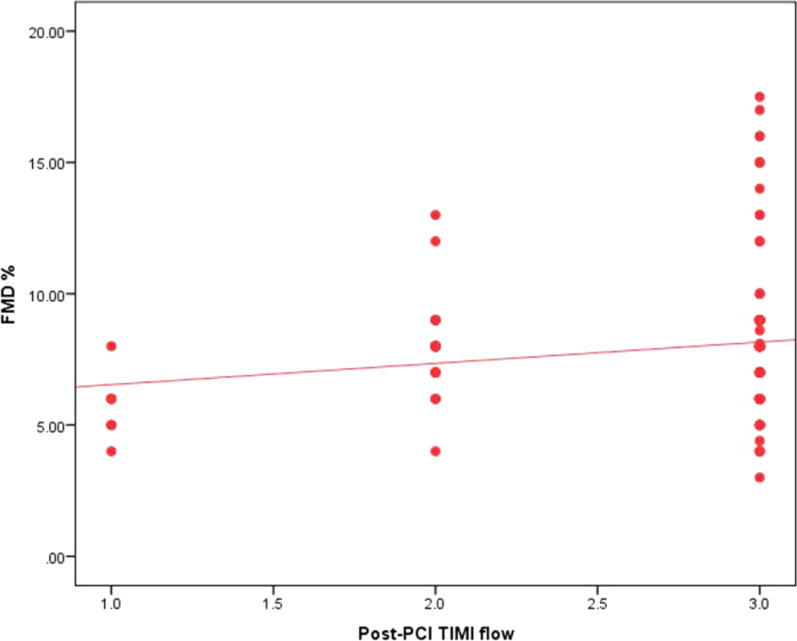
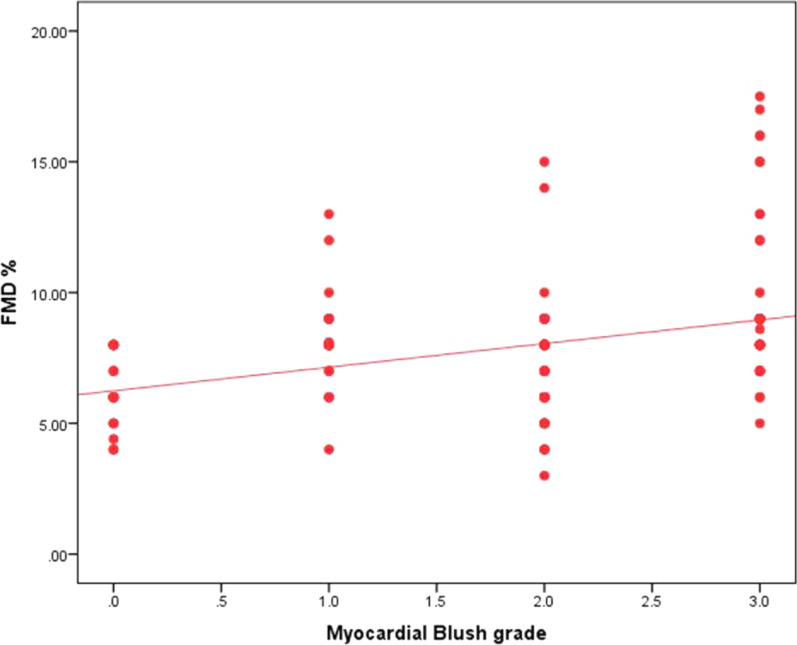
Results: This study included 150 patients managed by the percutaneous coronary intervention (PCI) after successful fibrinolysis. Patients were divided according to coronary angiographic success into normal flow versus no-reflow groups. According to FMD measured through brachial artery ultrasound, patients were divided based on their endothelial function into endothelial dysfunction versus normal endothelial function. No-reflow occurred in 44 patients (29.3%). No-reflow patients had longer pain to door time (6.52 ± 1.82 vs 5.19 ± 1.85 h), more Killip class II (36.4% vs 16%, p = 0.006), and lower FMD (7.26 ± 1.92 vs 8.23 ± 2.76%, p = 0.036). Also, they showed more endothelial dysfunction; however, this difference was statistically nonsignificant (97.7% vs 87.7%, p = 0.055). One hundred and thirty-six patients (90.7%) had endothelial dysfunction. They were older (57.51 ± 5.92 vs 50.86 ± 4.55 years, p value ≤ 0.001), more smokers (41.2% vs 14.3%, p = 0.04). Patients with normal endothelial function had a more myocardial blush grade (MBG) 3 (78.6% vs 26.5%, p value = 0.001) in comparison with more MBG 2 in those with endothelial dysfunction (41.9% vs 14.3%, p value = 0.001). Endothelial dysfunction patients had nonsignificant more no-reflow (31.6% vs 7.1%, p-value: 0.06). There was a significant weak positive correlation between thrombolysis in myocardial infarction (TIMI) flow and FMD (r = 0.174, p = 0.033) and a significant moderate positive correlation between MBG and FMD (r = 0.366, p < 0.001). Patients with TIMI I flow had significantly lower FMD compared with patients with TIMI II and TIMI III flow post-PCI. FMD ≤ 6% could predict post-procedural TIMI I flow.
Conclusions: In STEMI patients who underwent PCI within 24 h after successful fibrinolysis, those who had no-reflow showed worse peripheral systemic endothelial function as they had lower brachial artery FMD. Also, FMD showed a significant positive correlation with the post-procedural angiographic flow (TIMI flow and MBG). FMD ≤ 6% could predict TIMI I flow.
Keywords: Coronary intervention; Endothelial dysfunction; Fibrinolysis; Flow-mediated dilatation; Myocardial blush grade; Myocardial infarction; No-reflow; TIMI flow.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Mayyas F, Al-Jarrah M, Ibrahim K, Mfady D, Van Wagoner DR. The significance of circulating endothelin-1 as a predictor of coronary artery disease status and clinical outcomes following coronary artery catheterization. Cardiovasc Pathol. 2015;24(1):19–25. doi: 10.1016/j.carpath.2014.08.004. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous