

Consensus-Based Recommendations on Priority Activities to Address Acute Kidney Injury in Children: A Modified Delphi Consensus Statement
- PMID: 36178697
- PMCID: PMC9756303
- DOI: 10.1001/jamanetworkopen.2022.29442
Consensus-Based Recommendations on Priority Activities to Address Acute Kidney Injury in Children: A Modified Delphi Consensus Statement
Abstract
Importance: Increasing evidence indicates that acute kidney injury (AKI) occurs frequently in children and young adults and is associated with poor short-term and long-term outcomes. Guidance is required to focus efforts related to expansion of pediatric AKI knowledge.
Objective: To develop expert-driven pediatric specific recommendations on needed AKI research, education, practice, and advocacy.
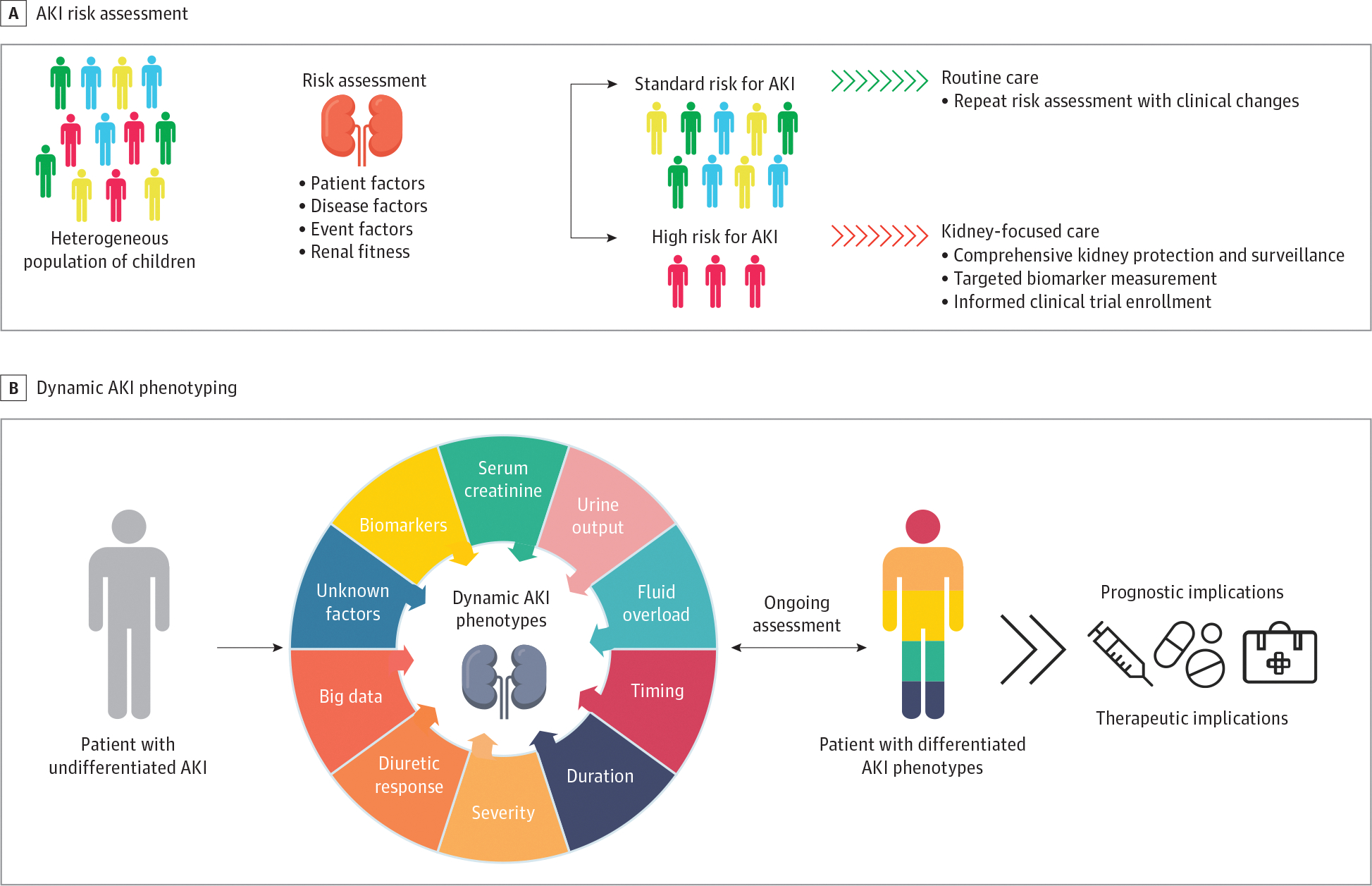
Evidence review: At the 26th Acute Disease Quality Initiative meeting conducted in November 2021 by 47 multiprofessional international experts in general pediatrics, nephrology, and critical care, the panel focused on 6 areas: (1) epidemiology; (2) diagnostics; (3) fluid overload; (4) kidney support therapies; (5) biology, pharmacology, and nutrition; and (6) education and advocacy. An objective scientific review and distillation of literature through September 2021 was performed of (1) epidemiology, (2) risk assessment and diagnosis, (3) fluid assessment, (4) kidney support and extracorporeal therapies, (5) pathobiology, nutrition, and pharmacology, and (6) education and advocacy. Using an established modified Delphi process based on existing data, workgroups derived consensus statements with recommendations.
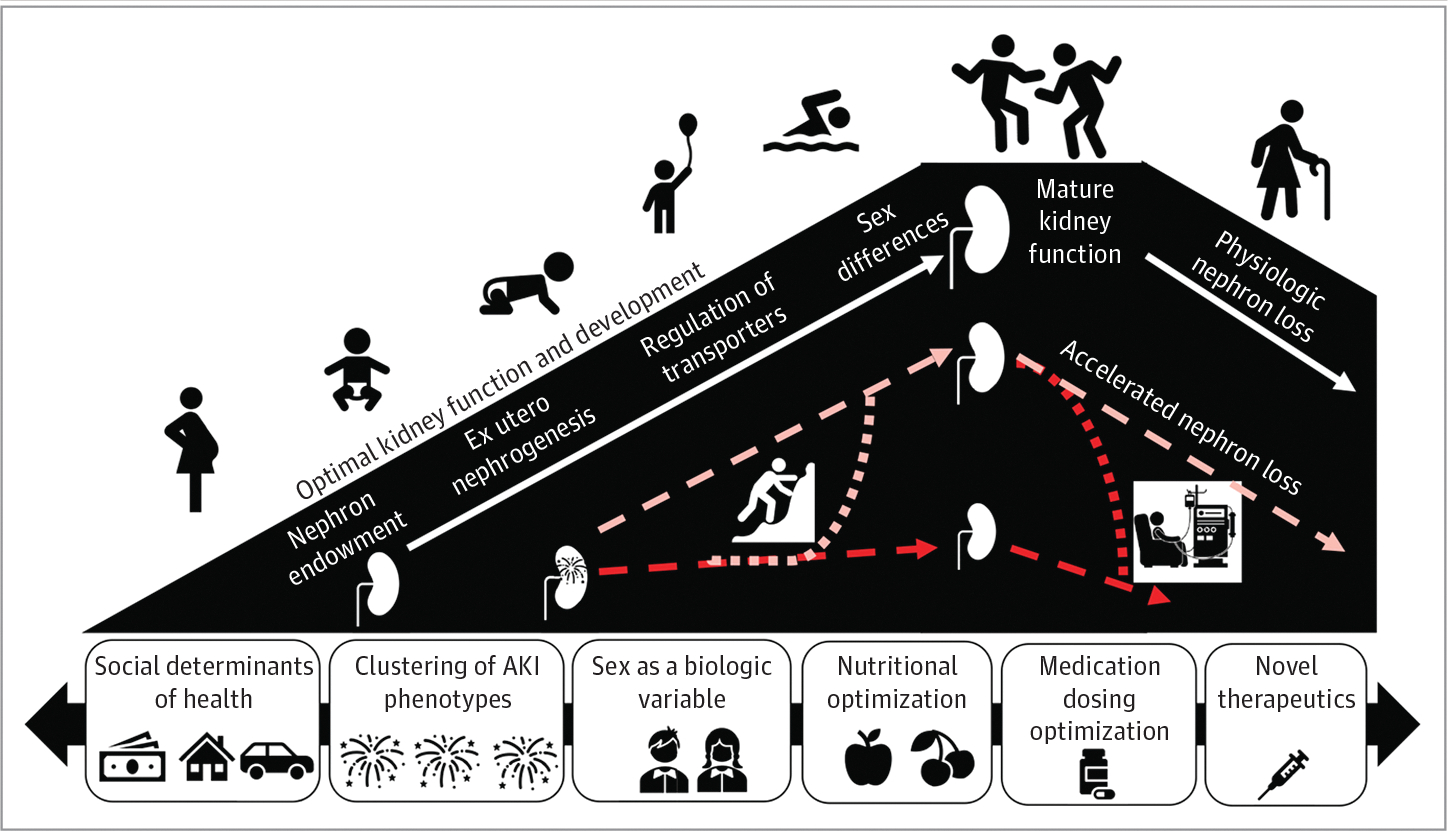
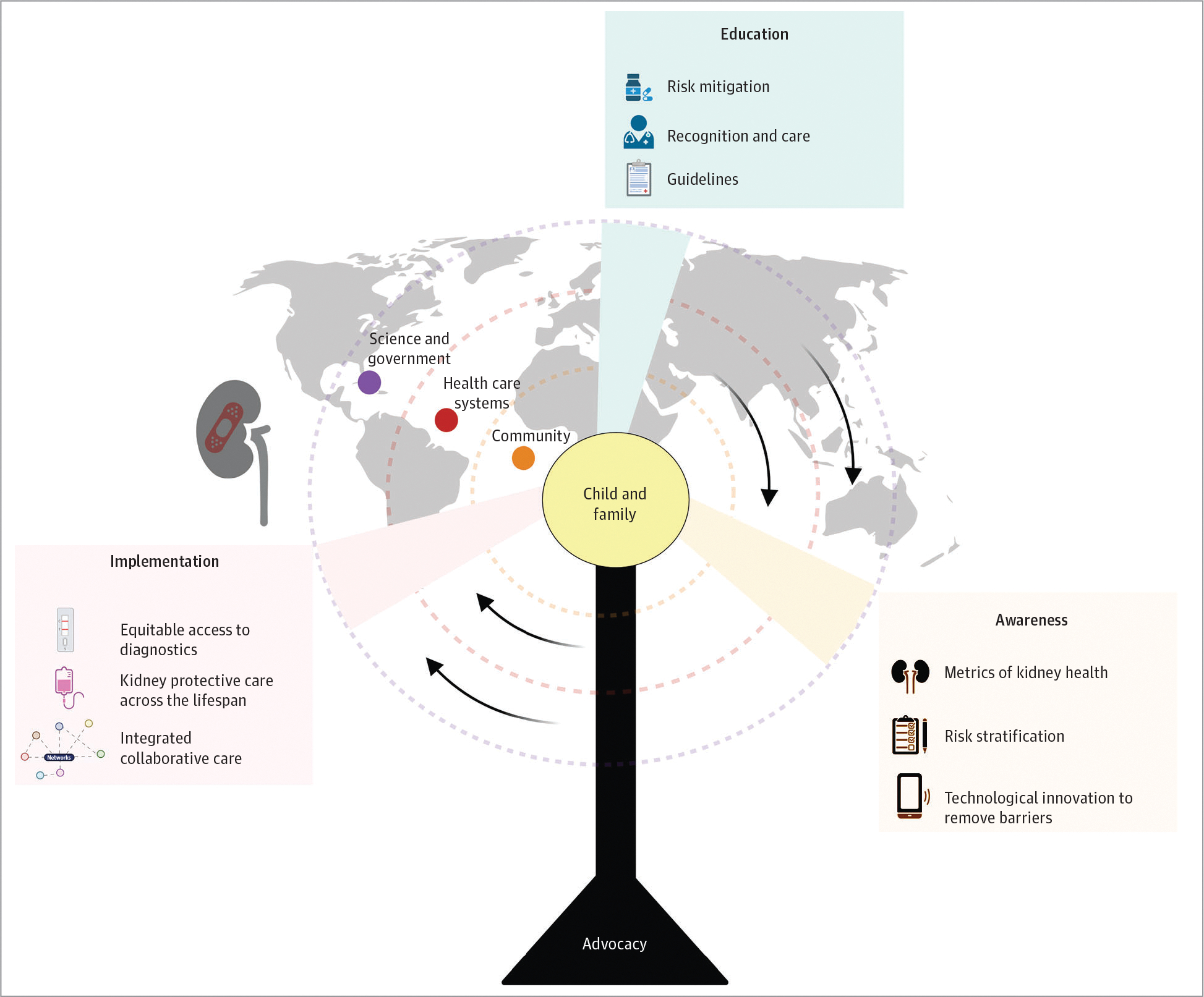
Findings: The meeting developed 12 consensus statements and 29 research recommendations. Principal suggestions were to address gaps of knowledge by including data from varying socioeconomic groups, broadening definition of AKI phenotypes, adjudicating fluid balance by disease severity, integrating biopathology of child growth and development, and partnering with families and communities in AKI advocacy.
Conclusions and relevance: Existing evidence across observational study supports further efforts to increase knowledge related to AKI in childhood. Significant gaps of knowledge may be addressed by focused efforts.
Conflict of interest statement
Figures
Comment in
-
Highlights of Consensus-Based Recommendations for Acute Kidney Injury in Children.JAMA Netw Open. 2022 Sep 1;5(9):e2229511. doi: 10.1001/jamanetworkopen.2022.29511. JAMA Netw Open. 2022. PMID: 36178696 No abstract available.
References
-
- Jetton JG, Boohaker LJ, Sethi SK, et al.; Neonatal Kidney Collaborative (NKC). Incidence and outcomes of neonatal acute kidney injury (AWAKEN): a multicentre, multinational, observational cohort study. Lancet Child Adolesc Health. 2017;1(3):184–194. doi:10.1016/S2352-4642(17)30069-X - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
