

Factors associated with in-hospital mortality of patients admitted to an intensive care unit in a tertiary hospital in Malawi
- PMID: 36178880
- PMCID: PMC9524689
- DOI: 10.1371/journal.pone.0273647
Factors associated with in-hospital mortality of patients admitted to an intensive care unit in a tertiary hospital in Malawi
Abstract
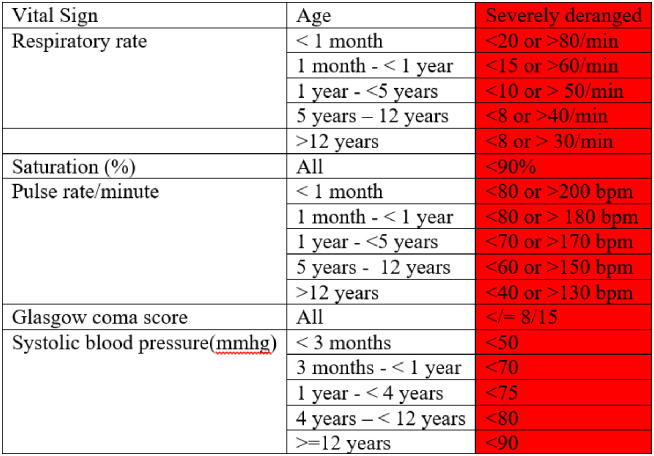
Objective: To determine factors associated with in-hospital death among patients admitted to ICU and to evaluate the predictive values of single severely deranged vital signs and several severity scoring systems.
Methods: A combined retrospective and prospective cohort study of patients admitted to the adult ICU in a tertiary hospital in Malawi was conducted between January 2017 and July 2019. Predefined potential risk factors for in-hospital death were studied with univariable and multivariable logistic regression models, and the performance of severity scores was assessed.
Results: The median age of the 822 participants was 31 years (IQR 21-43), and 50% were female. Several factors at admission were associated with in-hospital mortality: the presence of one or more severely deranged vital signs, adjusted odds ratio (aOR) 1.9 (1.4-2.6); treatment with vasopressor aOR 2.3 (1.6-3.4); received cardiopulmonary resuscitation aOR 1.7 (1.2-2.6) and treatment with mechanical ventilation aOR 1.5 (1.1-2.1). Having had surgery had a negative association with in-hospital mortality aOR 0.5 (0.4-0.7). The predictive accuracy of the severity scoring systems had varying sensitivities and specificities, but none were sufficiently accurate to be clinically useful.
Conclusions: In conclusion, the presence of one or more severely deranged vital sign in patients admitted to ICU may be useful as a simple marker of an increased risk of in-hospital death.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- McGinley A, Pearse RM. A national early warning score for acutely ill patients. Bmj.2012;345(aug081):e5310–e5310. http://www.bmj.com/cgi/doi/10.1136/bmj.e5310 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
