

Institutional factors associated with the incidence rates of central line-associated bloodstream infection in California community hospitals
- PMID: 36178895
- PMCID: PMC9524680
- DOI: 10.1371/journal.pone.0274436
Institutional factors associated with the incidence rates of central line-associated bloodstream infection in California community hospitals
Abstract
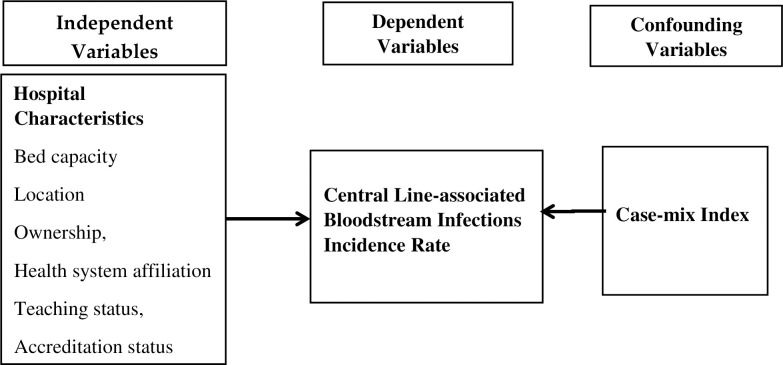
Central line-associated bloodstream infections are frequent, deadly, costly, and preventable. The study aimed to explore how some hospital-related characteristics were associated with incidence rates of central line-associated bloodstream infections reported by community hospitals in California from January to December 2019. This retrospective, cross-sectional study used combined data from records submitted to the California Department of Public Health, California Open Data Portal, the California Health and Human Services Open Data Portal, and the American Hospital Directory by community hospitals in California with central line-associated bloodstream infections in 2019. Results showed that CLABSIs are significantly associated with bed capacity, health care system affiliation, ownership, and hospital accreditation status (p < 0.0001). CLABSI remains a relevant threat to patient safety and quality of care, even more so in the community hospital setting. Understanding if a relationship exists between institutional factors and CLABSI rates might better prepare leaders in healthcare organizations to reduce HAIs.
Conflict of interest statement
The authors have declared that no competing interests exist.
References
-
- Kohn LT, Corrigan JM, Donaldson MS. To err is human: Building a safer health system. Washington (DC): The National Academies Press; 2000. 312 p. - PubMed
-
- Sax H, Pittet D, the Swiss-NOSO Network. Interhospital differences in nosocomial infection rates: Importance of case-mix adjustment. Arch Intern Med. 2002;162(21):2437–42. - PubMed
-
- U.S. Centers for Disease Control and Prevention. National Healthcare Safety Network (NHSN) Patient Safety Component Manual 2019.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
