

Ancestry-driven recalibration of tumor mutational burden and disparate clinical outcomes in response to immune checkpoint inhibitors
- PMID: 36179682
- PMCID: PMC9559771
- DOI: 10.1016/j.ccell.2022.08.022
Ancestry-driven recalibration of tumor mutational burden and disparate clinical outcomes in response to immune checkpoint inhibitors
Abstract
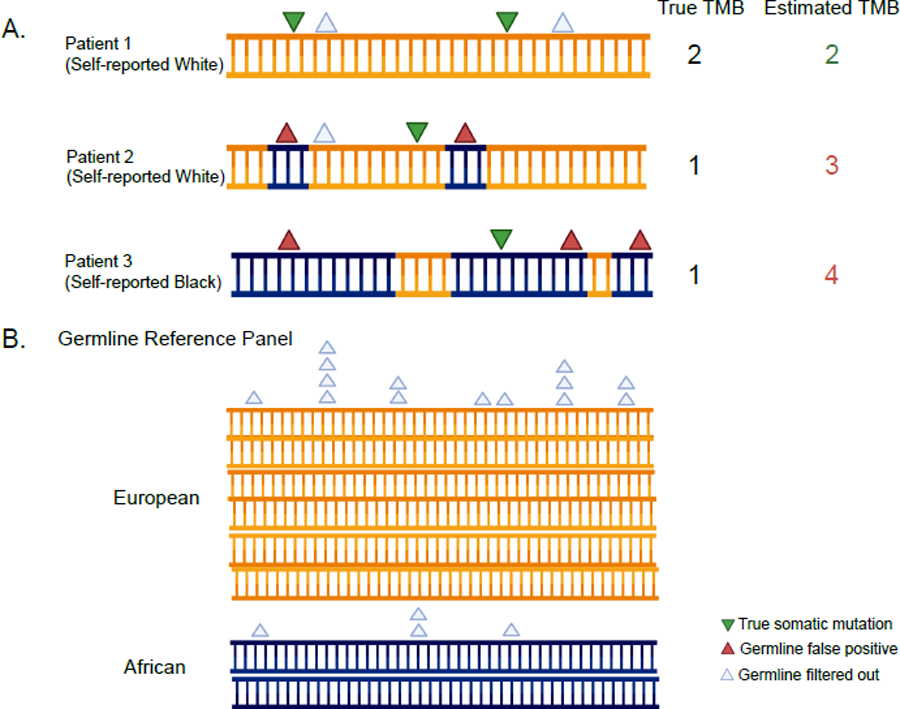
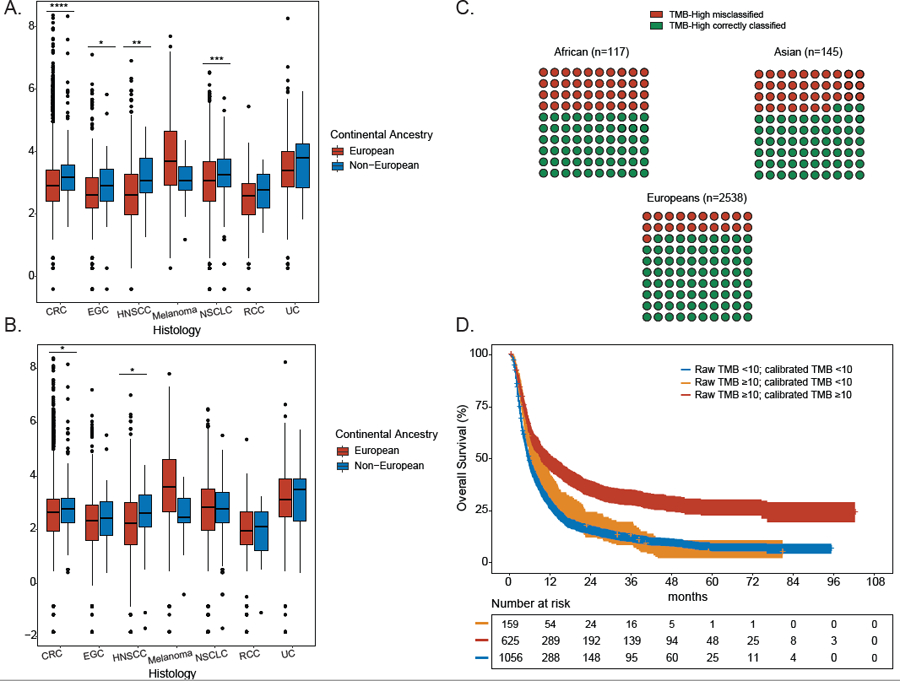
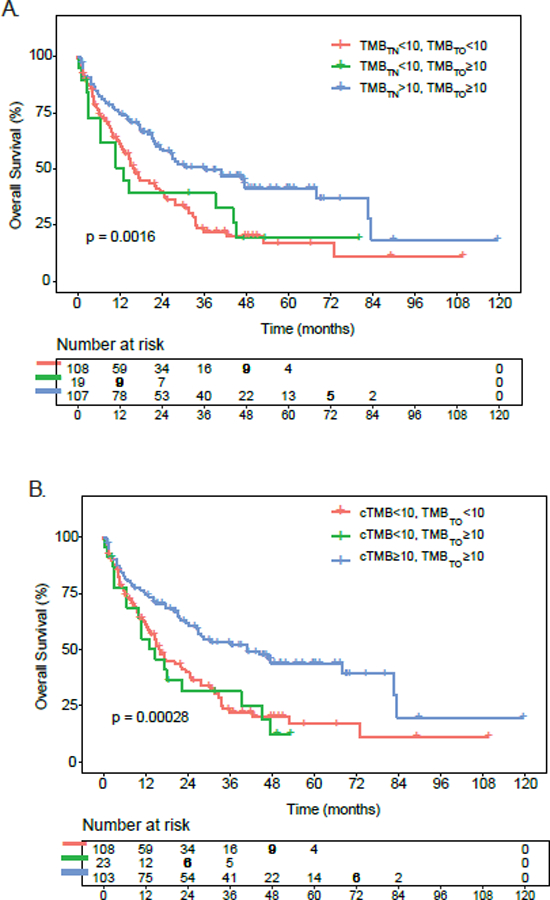
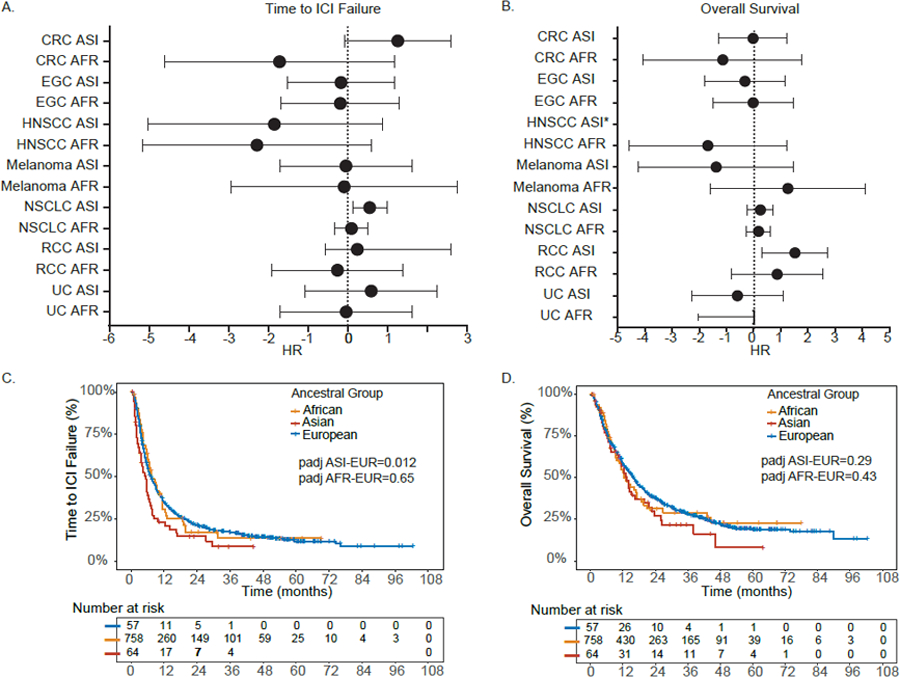
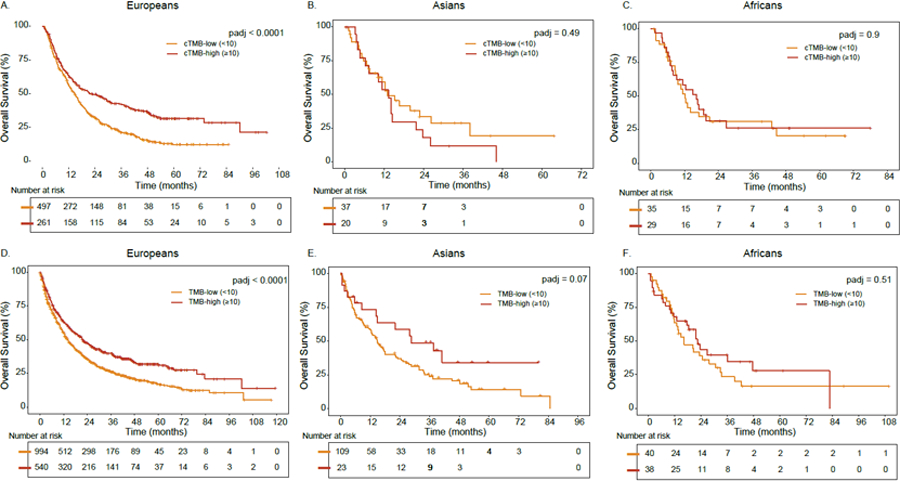
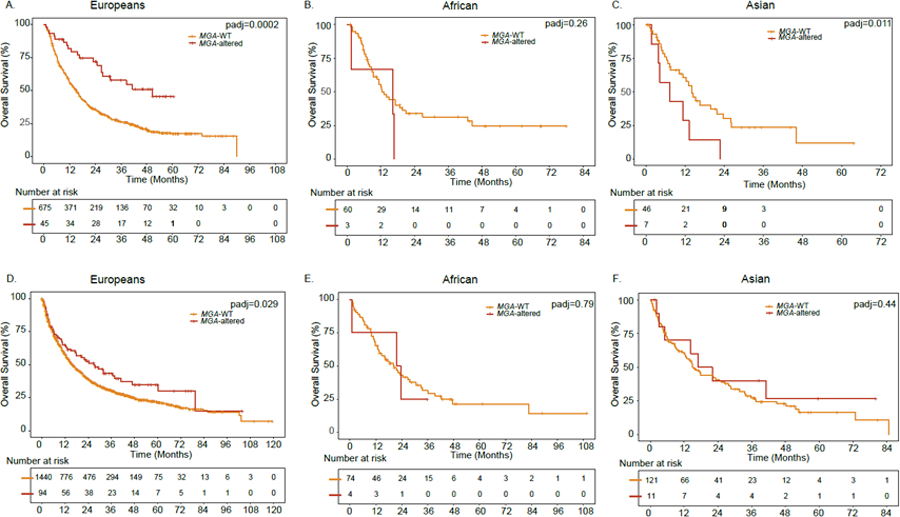
The immune checkpoint inhibitor (ICI) pembrolizumab is US FDA approved for treatment of solid tumors with high tumor mutational burden (TMB-high; ≥10 variants/Mb). However, the extent to which TMB-high generalizes as an accurate biomarker in diverse patient populations is largely unknown. Using two clinical cohorts, we investigated the interplay between genetic ancestry, TMB, and tumor-only versus tumor-normal paired sequencing in solid tumors. TMB estimates from tumor-only panels substantially overclassified individuals into the clinically important TMB-high group due to germline contamination, and this bias was particularly pronounced in patients with Asian/African ancestry. Among patients with non-small cell lung cancer treated with ICIs, those misclassified as TMB-high from tumor-only panels did not associate with improved outcomes. TMB-high was significantly associated with improved outcomes only in European ancestries and merits validation in non-European ancestry populations. Ancestry-aware tumor-only TMB calibration and ancestry-diverse biomarker studies are critical to ensure that existing disparities are not exacerbated in precision medicine.
Keywords: biomarker; cancer disparities; genetic ancestry; genomics; immunotherapy; tumor mutational burden.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests G.S. reports the following disclosures: advisory boards of BMS, Genentech, EMD Serono, Merck, Sanofi, Seattle Genetics/Astellas, Astrazeneca, Exelixis, Janssen, Bicycle Therapeutics, Pfizer, Immunomedics/Gilead, Scholar Rock, and G1 Therapeutics; research support to Sanofi, Astrazeneca, Immunomedics/Gilead, QED, Predicine, and BMS; steering committee of studies of BMS, Bavarian Nordic, Seattle Genetics, QED, and G1 Therapeutics (all unpaid) and Astrazeneca, EMD Serono, Debiopharm (paid); data safety monitoring committee of Mereo; travel costs from BMS (2019) and Astrazeneca (2018); writing/editor fees from UpToDate and as editor of the Elsevier PracticeUpdate Bladder Cancer Center of Excellence; speaking fees from Physicians Education Resource (PER), Onclive, Research to Practice, and Medscape (all educational). M.G. receives research funding from Bristol-Myers Squibb, Merck, Servier, and Janssen. F.S.H. reports grants and other from Bristol-Myers Squibb; personal fees from Merck; personal fees from EMD Serono; grants, personal fees, and other from Novartis; personal fees from Surface; personal fees from Compass Therapeutics; personal fees from Apricity; personal fees from Aduro; personal fees from Sanofi; personal fees from Pionyr; personal fees from Torque; personal fees from Bicara; other from Pieris Pharmaceuticals; personal fees from Eisai; personal fees from Checkpoint Therapeutics; personal fees from Idera; personal fees from Genentech/Roche; personal fees from BioEntre; personal fees from Gossamer; personal fees from Phio; personal fees from Iovance; personal fees from Trillium; personal fees from Abcuro; personal fees from Catalym; personal fees from Immunocore; outside the submitted work. In addition, F.S.H. has the following patents: Methods for Treating MICA-Related Disorders (20100111973) with royalties paid; Tumor Antigens and Uses Thereof (7250291) issued; Angiopoiten-2 Biomarkers Predictive of Anti-immune Checkpoint Response (20170248603) pending; Compositions and Methods for Identification, Assessment, Prevention, and Treatment of Melanoma using PD-L1 Isoforms (20160340407) pending; Therapeutic Peptides (20160046716) pending; Therapeutic Peptides (20140004112) pending; Therapeutic Peptides (20170022275) pending; Therapeutic Peptides (20170008962) pending; Therapeutic Peptides (9402905) issued; Methods of Using Pembrolizumab and Trebananib pending; Vaccine Compositions and Methods for Restoring NKG2D Pathway Function against Cancers (10279021) issued; Antibodies That Bind to MHC Class I Polypeptide-Related Sequence A (10106611) issued; and Anti-galectin Antibody Biomarkers Predictive of Anti-immune Checkpoint and Anti-angiogenesis Responses. T.K.C. reports the following disclosures: research/advisory boards/consultancy/honoraria (institutional and personal, paid and unpaid) for or from AstraZeneca, Aveo, Bayer, Bristol Myers-Squibb, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, IQVA, Ipsen, Kanaph, Lilly, Merck, Nikang, Novartis, Pfizer, Roche, Sanofi/Aventis, Takeda, and Tempest; travel, accommodations, expenses, medical writing in relation to consulting, advisory roles, or honoraria; stock options in Pionyr and Tempest; and other: UpToDate royalties, CME-related events (e.g., OncLIve, PVI, MJH Life Sciences) honoraria, NCI GU steering committee. T.K.C. also has patents filed, royalties, or other intellectual properties (no income as of this writing) related to biomarkers of immune checkpoint blockers and ctDNA. No speaker’s bureau. T.K.C. is supported in part by the Dana-Farber/Harvard Cancer Center Kidney SPORE and Program, the Kohlberg Chair at Harvard Medical School and the Trust Family, Michael Brigham, and Loker Pinard Funds for Kidney Cancer Research at DFCI.
Figures
Comment in
-
The importance of ancestry to understanding tumor mutation burden in cancer.Cancer Cell. 2022 Oct 10;40(10):1076-1078. doi: 10.1016/j.ccell.2022.09.004. Epub 2022 Sep 29. Cancer Cell. 2022. PMID: 36179683
-
Biomarker benchmarking.Nat Rev Genet. 2022 Dec;23(12):714. doi: 10.1038/s41576-022-00540-2. Nat Rev Genet. 2022. PMID: 36203016 No abstract available.
-
A refined use of mutations to guide immunotherapy decisions.Nature. 2022 Dec;612(7941):639-641. doi: 10.1038/d41586-022-04448-z. Nature. 2022. PMID: 36536222 No abstract available.
References
-
- (2020). AACR GENIE 8.0-public Data Guide In.
-
- Bach PB, Cramer LD, Schrag D, Downey RJ, Gelfand SE, and Begg CB (2001). The influence of hospital volume on survival after resection for lung cancer. N Engl J Med 345, 181–188. - PubMed
-
- Benjamin D, Sato T, Cibulskis K, Getz G, Stewart C, and Lichtenstein L (2019). Calling Somatic SNVs and Indels with Mutect2. bioRxiv, 861054
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
