

Toward a new taxonomy of obstetrical disease: improved performance of maternal blood biomarkers for the great obstetrical syndromes when classified according to placental pathology
- PMID: 36180175
- PMCID: PMC9525890
- DOI: 10.1016/j.ajog.2022.04.015
Toward a new taxonomy of obstetrical disease: improved performance of maternal blood biomarkers for the great obstetrical syndromes when classified according to placental pathology
Abstract
Background: The major challenge for obstetrics is the prediction and prevention of the great obstetrical syndromes. We propose that defining obstetrical diseases by the combination of clinical presentation and disease mechanisms as inferred by placental pathology will aid in the discovery of biomarkers and add specificity to those already known.
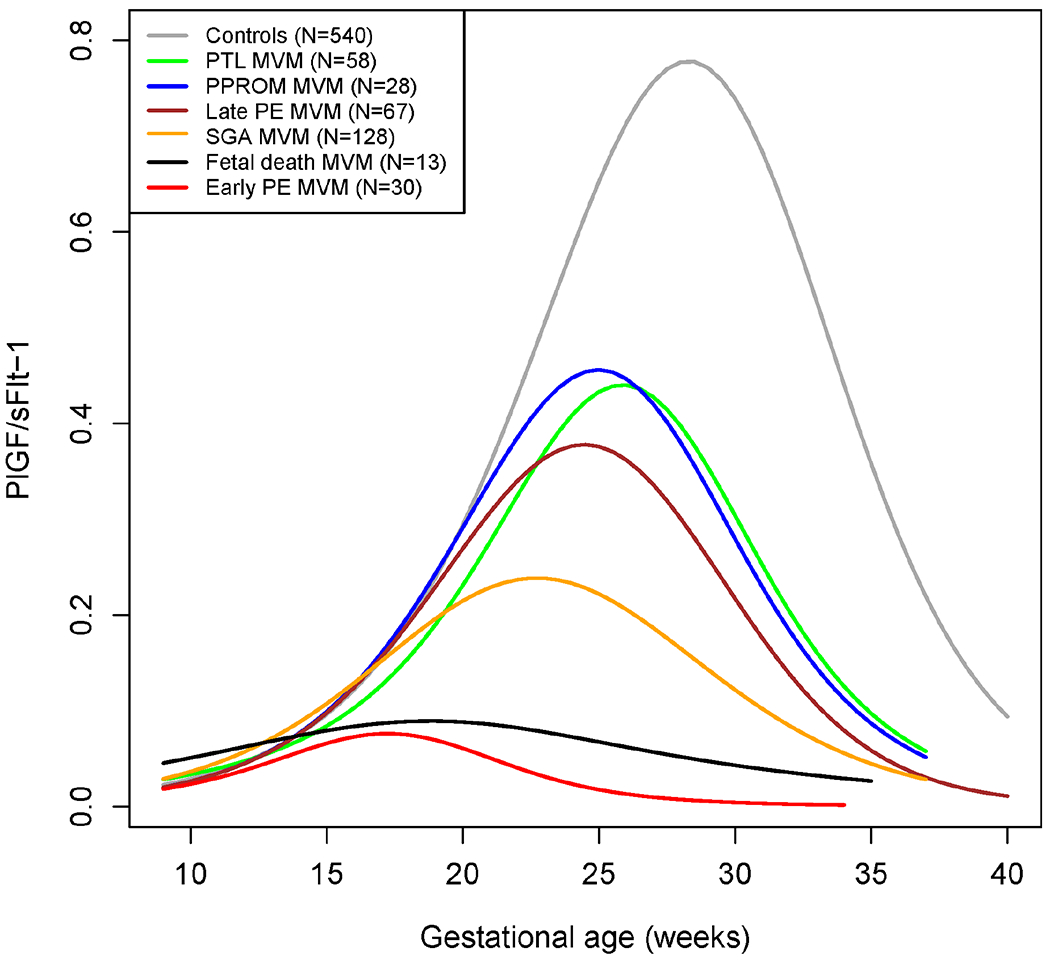
Objective: To describe the longitudinal profile of placental growth factor (PlGF), soluble fms-like tyrosine kinase-1 (sFlt-1), and the PlGF/sFlt-1 ratio throughout gestation, and to determine whether the association between abnormal biomarker profiles and obstetrical syndromes is strengthened by information derived from placental examination, eg, the presence or absence of placental lesions of maternal vascular malperfusion.
Study design: This retrospective case cohort study was based on a parent cohort of 4006 pregnant women enrolled prospectively. The case cohort of 1499 pregnant women included 1000 randomly selected patients from the parent cohort and all additional patients with obstetrical syndromes from the parent cohort. Pregnant women were classified into six groups: 1) term delivery without pregnancy complications (n=540; control); 2) preterm labor and delivery (n=203); 3) preterm premature rupture of the membranes (n=112); 4) preeclampsia (n=230); 5) small-for-gestational-age neonate (n=334); and 6) other pregnancy complications (n=182). Maternal plasma concentrations of PlGF and sFlt-1 were determined by enzyme-linked immunosorbent assays in 7560 longitudinal samples. Placental pathologists, masked to clinical outcomes, diagnosed the presence or absence of placental lesions of maternal vascular malperfusion. Comparisons between mean biomarker concentrations in cases and controls were performed by utilizing longitudinal generalized additive models. Comparisons were made between controls and each obstetrical syndrome with and without subclassifying cases according to the presence or absence of placental lesions of maternal vascular malperfusion.
Results: 1) When obstetrical syndromes are classified based on the presence or absence of placental lesions of maternal vascular malperfusion, significant differences in the mean plasma concentrations of PlGF, sFlt-1, and the PlGF/sFlt-1 ratio between cases and controls emerge earlier in gestation; 2) the strength of association between an abnormal PlGF/sFlt-1 ratio and the occurrence of obstetrical syndromes increases when placental lesions of maternal vascular malperfusion are present (adjusted odds ratio [aOR], 13.6 vs 6.7 for preeclampsia; aOR, 8.1 vs 4.4 for small-for-gestational-age neonates; aOR, 5.5 vs 2.1 for preterm premature rupture of the membranes; and aOR, 3.3 vs 2.1 for preterm labor (all P<0.05); and 3) the PlGF/sFlt-1 ratio at 28 to 32 weeks of gestation is abnormal in patients who subsequently delivered due to preterm labor with intact membranes and in those with preterm premature rupture of the membranes if both groups have placental lesions of maternal vascular malperfusion. Such association is not significant in patients with these obstetrical syndromes who do not have placental lesions.
Conclusion: Classification of obstetrical syndromes according to the presence or absence of placental lesions of maternal vascular malperfusion allows biomarkers to be informative earlier in gestation and enhances the strength of association between biomarkers and clinical outcomes. We propose that a new taxonomy of obstetrical disorders informed by placental pathology will facilitate the discovery and implementation of biomarkers as well as the prediction and prevention of such disorders.
Keywords: angiogenic index-1; classification of disease; fetal death; liquid biopsy; omics; placental growth factor; placental lesions of maternal vascular malperfusion; preeclampsia; pregnancy; preterm birth; preterm labor; preterm premature rupture of the membranes; small for gestational age; soluble fms-like tyrosine kinase-1; soluble vascular endothelial growth factor receptor-1.
Published by Elsevier Inc.
Conflict of interest statement
Figures







References
-
- Healthier mothers and babies. MMWR Morb Mortal Wkly Rep 1999;48:849–58. - PubMed
-
- Romero R Prevention of spontaneous preterm birth: the role of sonographic cervical length in identifying patients who may benefit from progesterone treatment. Ultrasound Obstet Gynecol 2007;30:675–86. - PubMed
-
- Fonseca EB, Celik E, Parra M, Singh M, Nicolaides KH, Fetal Medicine Foundation Second Trimester Screening G. Progesterone and the risk of preterm birth among women with a short cervix. N Engl J Med 2007;357:462–9. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
