

Effectiveness of COVID-19 vaccines against Omicron and Delta hospitalisation, a test negative case-control study
- PMID: 36180428
- PMCID: PMC9523190
- DOI: 10.1038/s41467-022-33378-7
Effectiveness of COVID-19 vaccines against Omicron and Delta hospitalisation, a test negative case-control study
Abstract
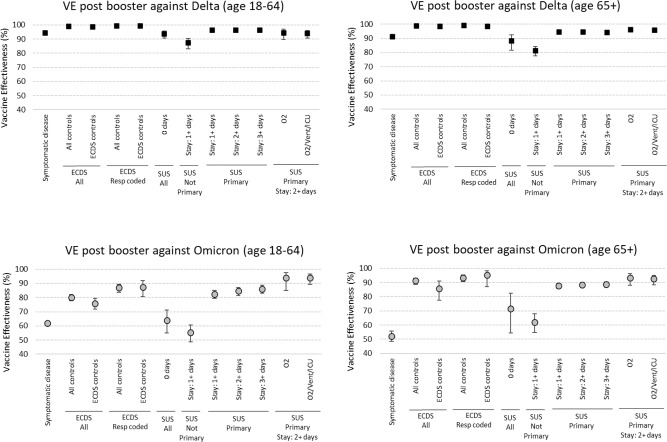
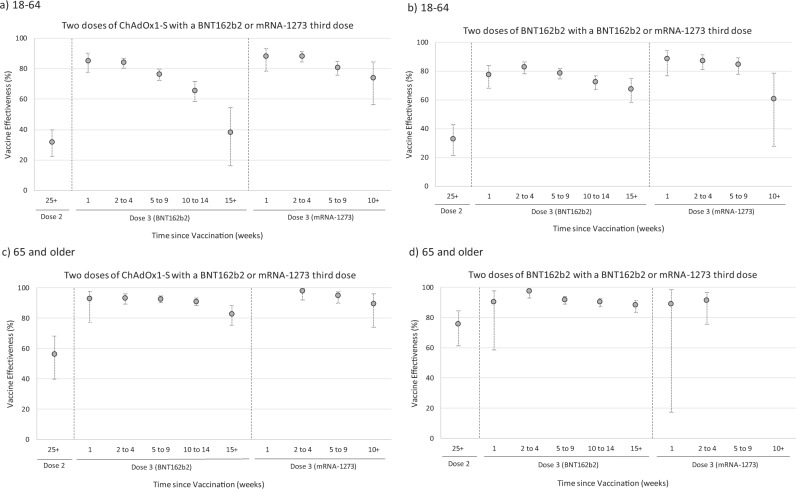
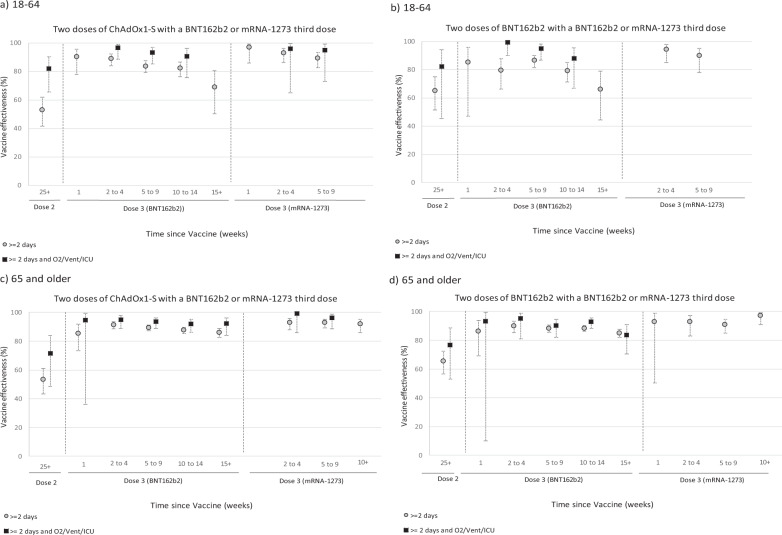
The Omicron variant has been associated with reduced vaccine effectiveness (VE) against mild disease with rapid waning. Meanwhile Omicron has also been associated with milder disease. Protection against severe disease has been substantially higher than protection against infection with previous variants. We used a test-negative case-control design to estimate VE against hospitalisation with the Omicron and Delta variants using PCR testing linked to hospital records. We investigated the impact of increasing the specificity and severity of hospitalisation definitions on VE. Among 18-64-year-olds using cases admitted via emergency care, VE after a 3rd dose peaked at 82.4% and dropped to 53.6% by 15+ weeks after the 3rd dose; using all admissions for > = 2 days stay with a respiratory code in the primary diagnostic field VE ranged from 90.9% to 67.4%; further restricting to those on oxygen/ventilated/intensive care VE ranged from 97.1% to 75.9%. Among 65+ year olds the equivalent VE estimates were 92.4% to 76.9%; 91.3% to 85.3% and 95.8% to 86.8%. Here we show that with milder Omicron disease contamination of hospitalisations with incidental cases is likely to reduce VE estimates. VE estimates increase, and waning is reduced, when specific hospitalisation definitions are used.
© 2022. Crown.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organization. COVID-19 Weekly Epidemiological Update, Edition 82 (World Health Organization, 2022).
-
- UK Health Security Agency. National flu and COVID-19 surveillance graphs: 10 March 2022 (week 10). https://www.gov.uk/government/statistics/national-flu-and-covid-19-surve... 2020.
-
- Cele, S. et al. SARS-CoV-2 Omicron has extensive but incomplete escape of Pfizer BNT162b2 elicited neutralization and requires ACE2 for infection. medRxiv [Preprint]. 2021.12.08.21267417, 10.1101/2021.12.08.21267417 (2021).
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
