

Cannulation configuration and recirculation in venovenous extracorporeal membrane oxygenation
- PMID: 36180496
- PMCID: PMC9523655
- DOI: 10.1038/s41598-022-20690-x
Cannulation configuration and recirculation in venovenous extracorporeal membrane oxygenation
Abstract
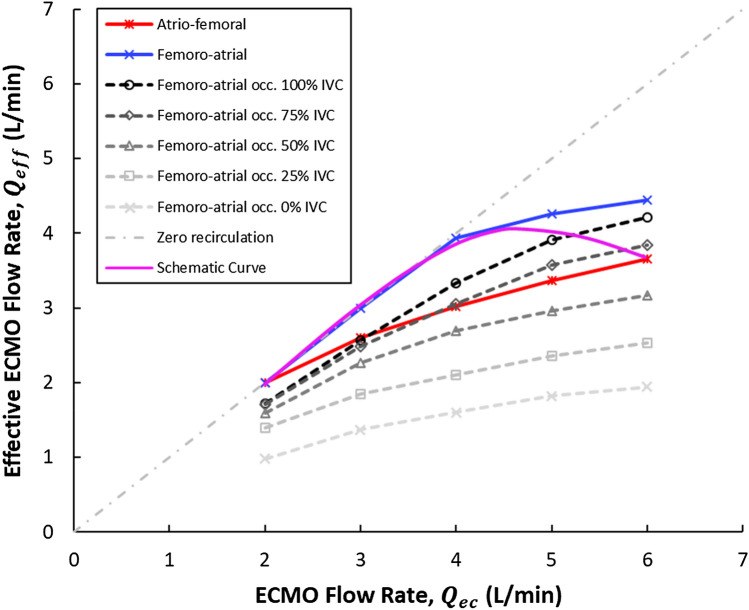
Venovenous extracorporeal membrane oxygenation is a treatment for acute respiratory distress syndrome. Femoro-atrial cannulation means blood is drained from the inferior vena cava and returned to the superior vena cava; the opposite is termed atrio-femoral. Clinical data comparing these two methods is scarce and conflicting. Using computational fluid dynamics, we aim to compare atrio-femoral and femoro-atrial cannulation to assess the impact on recirculation fraction, under ideal conditions and several clinical scenarios. Using a patient-averaged model of the venae cavae and right atrium, commercially-available cannulae were positioned in each configuration. Additionally, occlusion of the femoro-atrial drainage cannula side-holes with/without reduced inferior vena cava inflow (0-75%) and retraction of the atrio-femoral drainage cannula were modelled. Large-eddy simulations were run for 2-6L/min circuit flow, obtaining time-averaged flow data. The model showed good agreement with clinical atrio-femoral recirculation data. Under ideal conditions, atrio-femoral yielded 13.5% higher recirculation than femoro-atrial across all circuit flow rates. Atrio-femoral right atrium flow patterns resembled normal physiology with a single large vortex. Femoro-atrial cannulation resulted in multiple vortices and increased turbulent kinetic energy at > 3L/min circuit flow. Occluding femoro-atrial drainage cannula side-holes and reducing inferior vena cava inflow increased mean recirculation by 11% and 32%, respectively. Retracting the atrio-femoral drainage cannula did not affect recirculation. These results suggest that, depending on drainage issues, either atrio-femoral or femoro-atrial cannulation may be preferrable. Rather than cannula tip proximity, the supply of available venous blood at the drainage site appears to be the strongest factor affecting recirculation.
© 2022. The Author(s).
Conflict of interest statement
LMB is a member of the Medical Advisory Boards of Eurosets Srl., Medolla, Italy, and Xenios AG, Heilbronn, Germany.
Figures



References
-
- Barbaro RP, MacLaren G, Boonstra PS, Iwashyna TJ, Slutsky AS, Fan E, Bartlett RH, Tonna JE, Hyslop R, Fanning JJ, et al. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the extracorporeal life support organization registry. The Lancet. 2020;396(10257):1071–1078. doi: 10.1016/S0140-6736(20)32008-0. - DOI - PMC - PubMed
-
- Identification and management of recirculation in venovenous ECMO. In: Ann Arbor, MI, USA: Extracorporeal Life Support Organization (2015).
-
- Annich, G. M., Lynch, W. R., MacLaren, G., Wilson, J. M. & Bartlett, R.H. Ecmo: Extracorporeal cardiopulmonary support in critical care. (2018).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
