

A randomized prospective cross over study on the effects of medium cut-off membranes on T cellular and serologic immune phenotypes in hemodialysis
- PMID: 36180564
- PMCID: PMC9524345
- DOI: 10.1038/s41598-022-20818-z
A randomized prospective cross over study on the effects of medium cut-off membranes on T cellular and serologic immune phenotypes in hemodialysis
Abstract
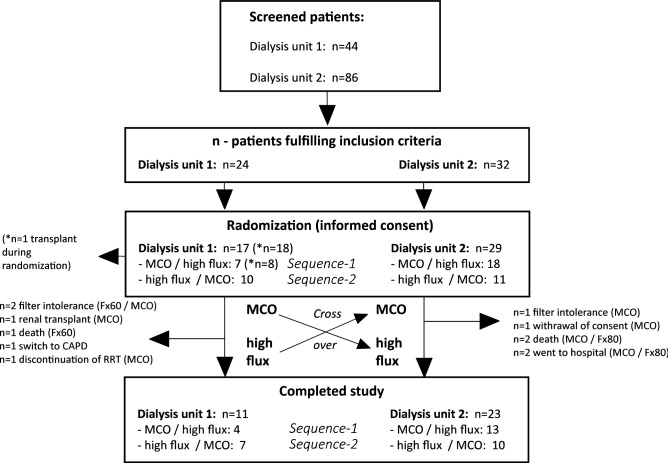
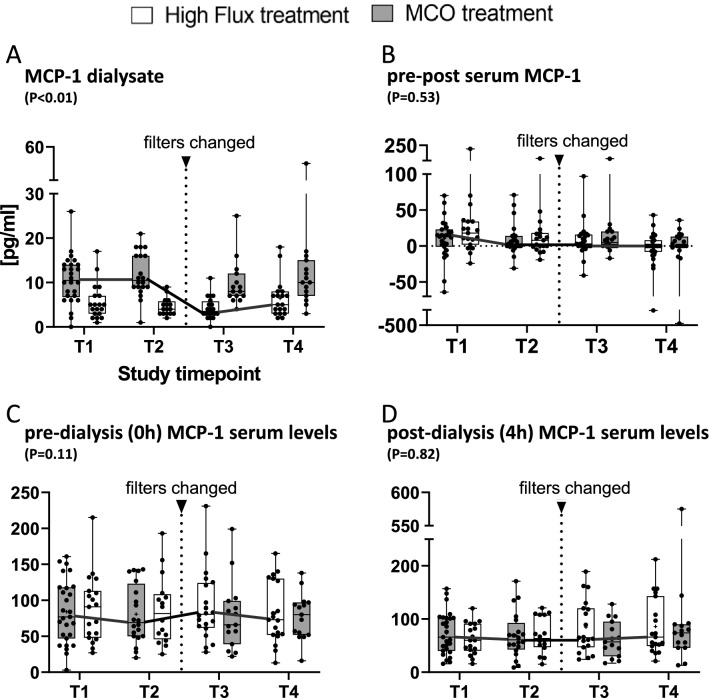
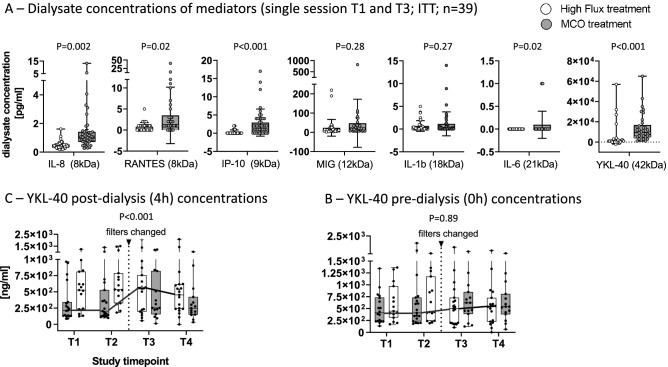
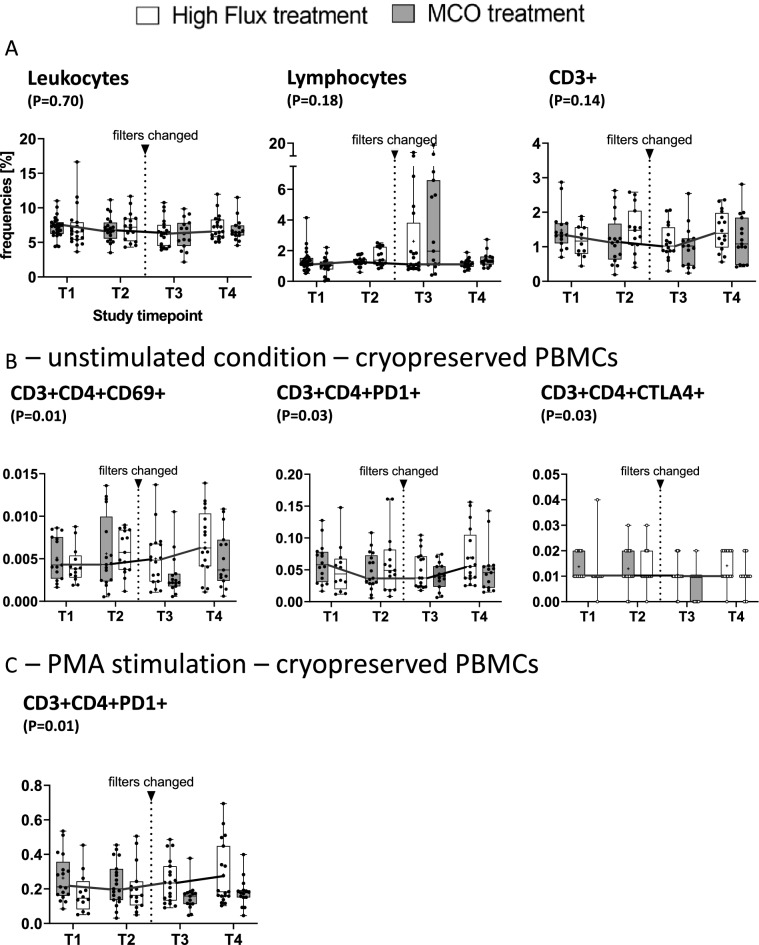
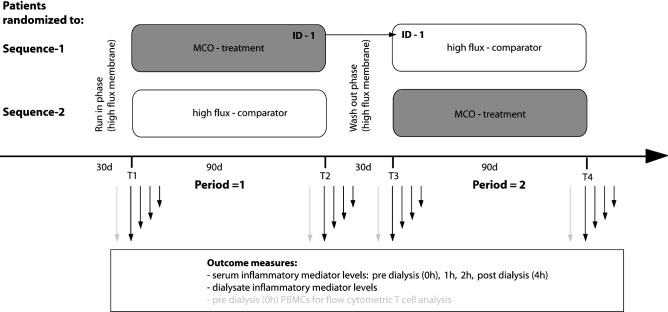
Extended cut-off filtration by medium cut-off membranes (MCO) has been shown to be safe in maintenance hemodialysis (HD). The notion of using them for the control of chronic low-grade inflammation and positively influencing cellular immune aberrations seems tempting. We conducted an open label, multicenter, randomized, 90 day 2-phase cross over clinical trial (MCO- vs. high flux-HD). 46 patients underwent randomization of which 34 completed the study. Dialysate- or pre- and post-dialysis serum inflammatory mediators were assayed for each study visit. Ex vivo T cell activation was assessed from cryopreserved leucocytes by flow cytometry. Linear mixed models were used to compare treatment modalities, with difference in pre-dialysis serum MCP-1 levels after 3 months as the predefined primary endpoint. Filtration/dialysate concentrations of most mediators, including MCP-1 (mean ± SD: 10.5 ± 5.9 vs. 5.1 ± 3.8 pg/ml, P < 0.001) were significantly increased during MCO- versus high flux-HD. However, except for the largest mediator studied, i.e., YKL-40, this did not confer any advantages for single session elimination kinetics (post-HD mean ± SD: 360 ± 334 vs. 564 ± 422 pg/ml, P < 0.001). No sustained reduction of any of the studied mediators was found neither. Still, the long-term reduction of CD69+ (P = 0.01) and PD1+ (P = 0.02) activated CD4+ T cells was striking. Thus, MCO-HD does not induce reduction of a broad range of inflammatory mediators studied here. Long-term reduction over a 3-month period was not possible. Increased single session filtration, as evidenced by increased dialysate concentrations of inflammatory mediators during MCO-HD, might eventually be compensated for by compartment redistribution or increased production during dialysis session. Nevertheless, lasting effects on the T-cell phenotype were seen, which deserves further investigation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
