

Clinico-radiological nomogram for preoperatively predicting post-resection hepatic metastasis in patients with gastric adenocarcinoma
- PMID: 36181505
- PMCID: PMC9733617
- DOI: 10.1259/bjr.20220488
Clinico-radiological nomogram for preoperatively predicting post-resection hepatic metastasis in patients with gastric adenocarcinoma
Abstract
Objective: To establish and validate a model comprising clinical and radiological features to pre-operatively predict post-resection hepatic metastasis (HM) in patients with gastric adenocarcinoma (GAC).
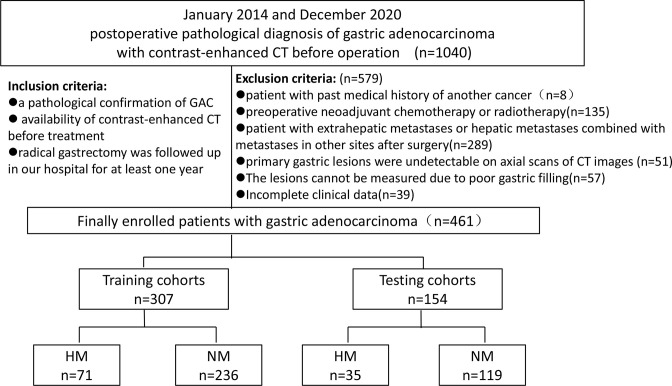
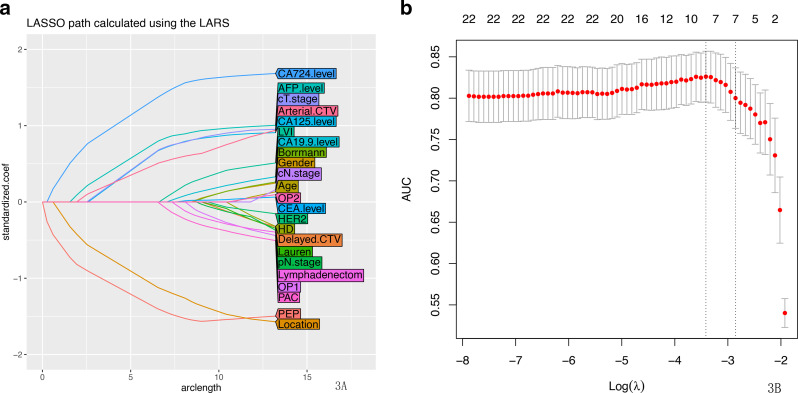
Methods: We retrospectively analyzed 461 patients (HM, 106 patients); and non-metastasis (NM, 355 patients) who were confirmed to have GAC post-surgery. The patients were randomly divided into the training (n = 307) and testing (n = 154) cohorts in a 2:1 ratio. The main clinical risk factors were filtered using the least absolute shrinkage and selection operator algorithm according to their diagnostic value. The selected factors were then used to establish a clinical-radiological model using stepwise logistic regression. The Akaike's information criterion and receiver operating characteristic (ROC) analyses were used to evaluate the prediction performance of the model.
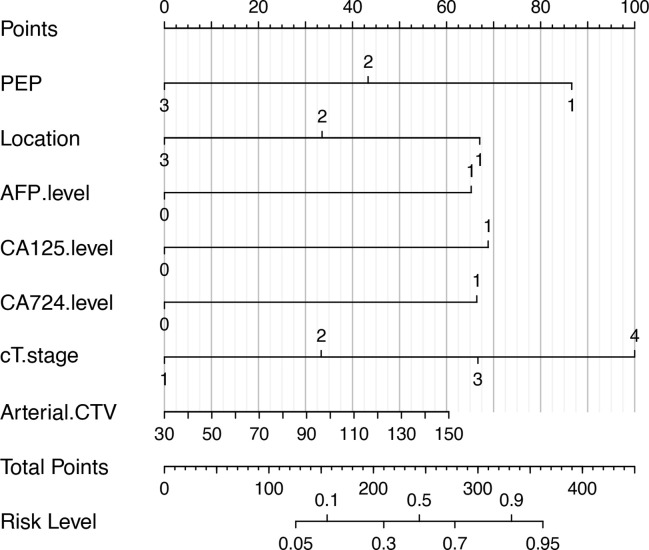
Results: Logistic regression analysis showed that the peak enhancement phase, tumor location, alpha-fetoprotein, cancer antigen (CA)-125, CA724 levels, CT-based Tstage and arterial phase CT values were important independent predictors. Based on these predictors, the areas under the ROC curve of the training and testing cohorts were 0.864 and 0.832, respectively, for predicting post-operative HM.
Conclusion: This study built a synthetical nomogram using the pre-operative clinical and radiological features of patients to predict the likelihood of HM occurring after GAC surgery. It may help guide pre-operative clinical decision-making and benefit patients with GAC in the future.
Advances in knowledge: 1. The combination of clinical risk factors and CT imaging features provided useful information for predicting HM in GAC.2. A clinicoradiological nomogram is a tool for the pre-operative prediction of HM in patients with GAC.
Figures
Similar articles
-
Preoperative prediction for lauren type of gastric cancer: A radiomics nomogram analysis based on CT images and clinical features.J Xray Sci Technol. 2021;29(4):675-686. doi: 10.3233/XST-210888. J Xray Sci Technol. 2021. PMID: 34024809 Clinical Trial.
-
Radiomics signature for predicting postoperative disease-free survival of patients with gastric cancer: development and validation of a predictive nomogram.Diagn Interv Radiol. 2022 Sep;28(5):441-449. doi: 10.5152/dir.2022.211034. Diagn Interv Radiol. 2022. PMID: 36097638 Free PMC article. Clinical Trial.
-
CT radiomics nomogram for the preoperative prediction of lymph node metastasis in gastric cancer.Eur Radiol. 2020 Feb;30(2):976-986. doi: 10.1007/s00330-019-06398-z. Epub 2019 Aug 29. Eur Radiol. 2020. PMID: 31468157
-
CT-based radiomics nomogram for differentiating gastric hepatoid adenocarcinoma from gastric adenocarcinoma: a multicentre study.Expert Rev Gastroenterol Hepatol. 2023 Feb;17(2):205-214. doi: 10.1080/17474124.2023.2166490. Epub 2023 Jan 18. Expert Rev Gastroenterol Hepatol. 2023. PMID: 36625225
-
Nomogram for predicting the survival of gastric adenocarcinoma patients who receive surgery and chemotherapy.BMC Cancer. 2020 Jan 6;20(1):10. doi: 10.1186/s12885-019-6495-2. BMC Cancer. 2020. PMID: 31906882 Free PMC article.
Cited by
-
Combining radiomics and deep learning to predict liver metastasis of gastric cancer on CT image.Front Oncol. 2025 Jun 24;15:1613972. doi: 10.3389/fonc.2025.1613972. eCollection 2025. Front Oncol. 2025. PMID: 40630210 Free PMC article.
-
Combination of clinical and spectral-CT iodine concentration for predicting liver metastasis in gastric cancer: a preliminary study.Abdom Radiol (NY). 2024 Oct;49(10):3438-3449. doi: 10.1007/s00261-024-04346-0. Epub 2024 May 15. Abdom Radiol (NY). 2024. PMID: 38744700
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
