

Physiological-based cord clamping in very preterm infants: the Aeration, Breathing, Clamping 3 (ABC3) trial-study protocol for a multicentre randomised controlled trial
- PMID: 36183143
- PMCID: PMC9526936
- DOI: 10.1186/s13063-022-06789-6
Physiological-based cord clamping in very preterm infants: the Aeration, Breathing, Clamping 3 (ABC3) trial-study protocol for a multicentre randomised controlled trial
Abstract
Background: International guidelines recommend delayed umbilical cord clamping (DCC) up to 1 min in preterm infants, unless the condition of the infant requires immediate resuscitation. However, clamping the cord prior to lung aeration may severely limit circulatory adaptation resulting in a reduction in cardiac output and hypoxia. Delaying cord clamping until lung aeration and ventilation have been established (physiological-based cord clamping, PBCC) allows for an adequately established pulmonary circulation and results in a more stable circulatory transition. The decline in cardiac output following time-based delayed cord clamping (TBCC) may thus be avoided. We hypothesise that PBCC, compared to TBCC, results in a more stable transition in very preterm infants, leading to improved clinical outcomes. The primary objective is to compare the effect of PBCC on intact survival with TBCC.
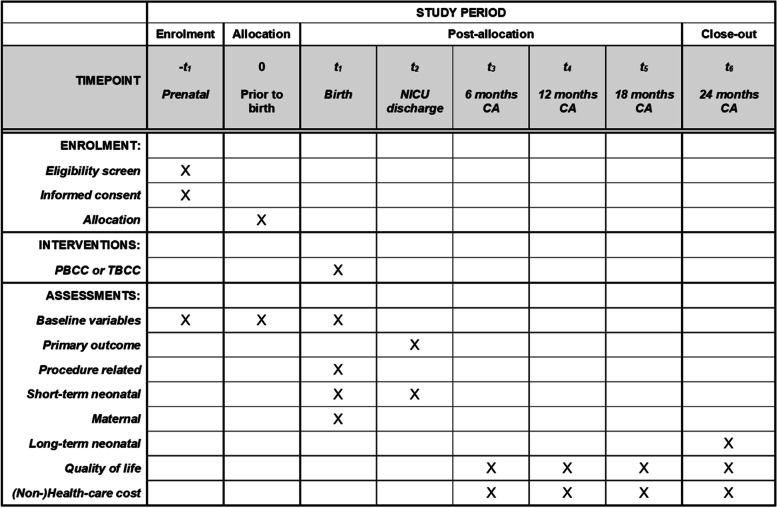
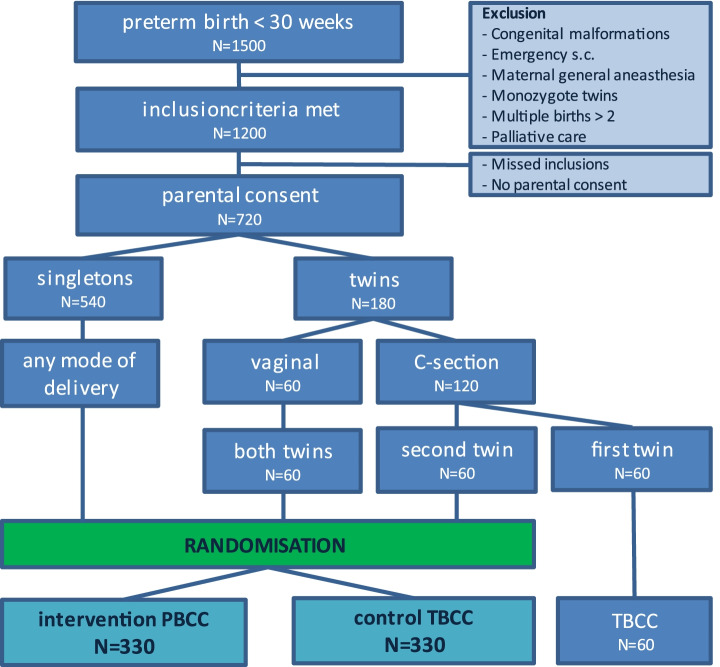
Methods: The Aeriation, Breathing, Clamping 3 (ABC3) trial is a multicentre randomised controlled clinical trial. In the interventional PBCC group, the umbilical cord is clamped after the infant is stabilised, defined as reaching heart rate > 100 bpm and SpO2 > 85% while using supplemental oxygen < 40%. In the control TBCC group, cord clamping is time based at 30-60 s. The primary outcome is survival without major cerebral and/or intestinal injury. Preterm infants born before 30 weeks of gestation are included after prenatal parental informed consent. The required sample size is 660 infants.
Discussion: The findings of this trial will provide evidence for future clinical guidelines on optimal cord clamping management in very preterm infants at birth.
Trial registration: ClinicalTrials.gov NCT03808051. First registered on January 17, 2019.
Keywords: Cord clamping; Physiological-based cord clamping; Preterm infants; Randomised clinical trial; Study protocol.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests. The Concords used in this trial were either designed and built by LUMC (for 3 participating centres) or purchased from Concord Neonatal B.V. (Leiden, The Netherlands; for 6 participating centres). ABtP, SBH and AHvK are members of the Scientific Advisory Board of Concord Neonatal B.V., but have no financial relationship or support. The company has no role in the design of the study; in the collection, analysis or interpretation of the data; or in the writing of the manuscript.
Figures


Similar articles
-
Physiological-based cord clamping in very preterm infants: the Aeration, Breathing, Clamping 3 (ABC3) trial-statistical analysis plan for a multicenter randomized controlled trial.Trials. 2024 Mar 4;25(1):164. doi: 10.1186/s13063-024-08014-y. Trials. 2024. PMID: 38439024 Free PMC article. Clinical Trial.
-
Physiological versus time based cord clamping in very preterm infants (ABC3): a parallel-group, multicentre, randomised, controlled superiority trial.Lancet Reg Health Eur. 2024 Dec 4;48:101146. doi: 10.1016/j.lanepe.2024.101146. eCollection 2025 Jan. Lancet Reg Health Eur. 2024. PMID: 39717227 Free PMC article.
-
Physiologically based cord clamping for infants ≥32+0 weeks gestation: A randomised clinical trial and reference percentiles for heart rate and oxygen saturation for infants ≥35+0 weeks gestation.PLoS Med. 2022 Jun 23;19(6):e1004029. doi: 10.1371/journal.pmed.1004029. eCollection 2022 Jun. PLoS Med. 2022. PMID: 35737735 Free PMC article. Clinical Trial.
-
Deferred cord clamping, cord milking, and immediate cord clamping at preterm birth: a systematic review and individual participant data meta-analysis.Lancet. 2023 Dec 9;402(10418):2209-2222. doi: 10.1016/S0140-6736(23)02468-6. Epub 2023 Nov 14. Lancet. 2023. PMID: 37977169
-
Clinical aspects of incorporating cord clamping into stabilisation of preterm infants.Arch Dis Child Fetal Neonatal Ed. 2018 Sep;103(5):F493-F497. doi: 10.1136/archdischild-2018-314947. Epub 2018 Apr 21. Arch Dis Child Fetal Neonatal Ed. 2018. PMID: 29680790 Free PMC article. Review.
Cited by
-
Umbilical cord management in newborn resuscitation: a systematic review and meta-analysis.Pediatr Res. 2025 Apr;97(5):1481-1491. doi: 10.1038/s41390-024-03496-7. Epub 2024 Sep 2. Pediatr Res. 2025. PMID: 39223253 Free PMC article.
-
Maternal implications of placental transfusion.Semin Perinatol. 2023 Jun;47(4):151733. doi: 10.1016/j.semperi.2023.151733. Epub 2023 Mar 17. Semin Perinatol. 2023. PMID: 37068968 Free PMC article.
-
The Respiratory Management of the Extreme Preterm in the Delivery Room.Children (Basel). 2023 Feb 10;10(2):351. doi: 10.3390/children10020351. Children (Basel). 2023. PMID: 36832480 Free PMC article. Review.
-
Physiological-Based Cord Clamping: When the Baby Is Ready for Clamping.Neonatology. 2024;121(5):547-552. doi: 10.1159/000540667. Epub 2024 Aug 28. Neonatology. 2024. PMID: 39197438 Free PMC article. Review.
-
Ventilatory Assistance Before Umbilical Cord Clamping in Extremely Preterm Infants: A Randomized Clinical Trial.JAMA Netw Open. 2024 May 1;7(5):e2411140. doi: 10.1001/jamanetworkopen.2024.11140. JAMA Netw Open. 2024. PMID: 38758557 Free PMC article. Clinical Trial.
References
-
- Mian Q, Cheung PY, O'Reilly M, Barton SK, Polglase GR, Schmolzer GM. Impact of delivered tidal volume on the occurrence of intraventricular haemorrhage in preterm infants during positive pressure ventilation in the delivery room. Arch Dis Child Fetal Neonatal Ed. 2019;104(1):F57–F62. doi: 10.1136/archdischild-2017-313864. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
