

Long-term outcomes of kidney transplantation from expanded criteria donors with Chinese novel donation policy: donation after citizens' death
- PMID: 36184632
- PMCID: PMC9528130
- DOI: 10.1186/s12882-022-02944-y
Long-term outcomes of kidney transplantation from expanded criteria donors with Chinese novel donation policy: donation after citizens' death
Abstract
Introduction: The Chinese Government initiated the Donation after Citizens' Death policy in 2010. To now, it has been a major source of organs for transplant. Since it is still a young policy, corresponding clinical evidence is still urgently needed for its improvement. Compared to kidneys donated by SCD (standard criteria donor), increasing the use of ECD (expanded criteria donor) derived kidneys is a way to expand the donor pool but is also a result of the aging demography of China. This study is based on the data of kidney transplantation in our center with the Donation after Citizens' Death policy, aiming to provide a reference for the clinical use of ECD kidneys.
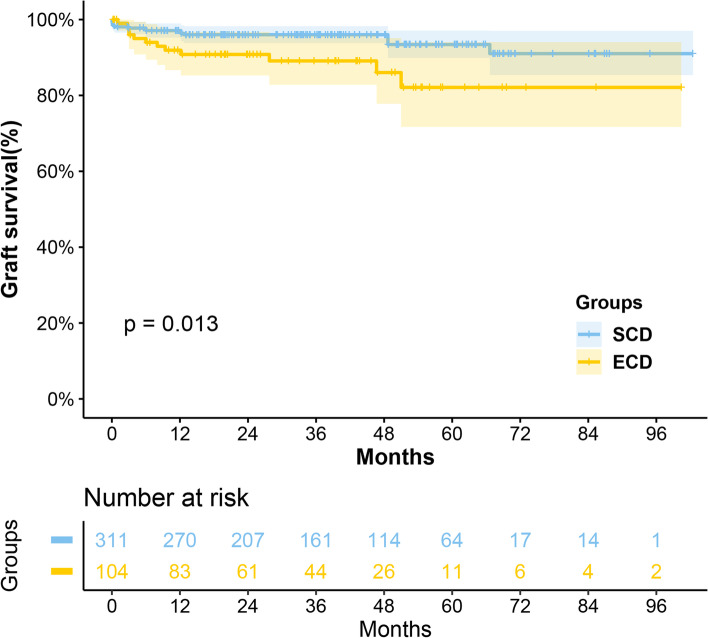
Method: A retrospective study enrolled 415 kidney transplants derived from 211 donors performed between October 2011 and October 2019. A total of 311 (74.9%) organs were donated from 159 (75.4%) SCDs, and the remaining 104 (25.1%) were from 52 (24.6%) ECDs. The log-rank test was used to compare the difference in survival and postoperative complications. The Chi-square test was used to compare the occurrence of postoperative complications and postoperative renal function. The Cox regression analysis was used for risk factor screening.
Result: Analysis showed that grafts from ECD were poorer in survival (P = 0.013), while their recipients had comparable (P = 0.16) survival. Moreover, it also was an independent risk factor for graft loss (HR 2.27, P = 0.044). There were significantly more AR occurrences in the ECD group compared with SCD group (25.0% vs. 15.8%, P = 0.004), but no significant difference was found in infection (51.9% vs. 47.6%, P = 0.497) and DGF (26.0% vs. 21.9%, P = 0.419) between them. Similarly, fewer recipients in the ECD group were free from AR within 1 year after transplantation (P = 0.040), with no statistical difference in all-cause infection prevalence in 1 year (P = 0.168). The eGFR in the ECD group was significantly worse than that in the SCD group at 3 months, 6 months, 1 year, 3 years, and the highest value posttransplant (all < 0.05), but no difference at 5 years posttransplant. Besides, results showed cardiac arrest (uncontrolled vs. controlled, HR 2.49, P = 0.049), HLA mismatch (4-6 loci vs. 0-3 loci, HR 3.61, P = 0.039), and AR occurrence (HR 2.91, P = 0.006) were demonstrated to be independent risk factors for graft loss.
Conclusion: The ECD-derived kidney was worse than the SCD-derived kidney in terms of graft survival and AR occurrence, and trend to an inferior renal function postoperative. However, the recipient survival, DGF occurrence, and all-cause infection occurrence were similar.
Keywords: Donation after Citizens’ Death; Expended criteria donor; Kidney transplantation; Outcomes.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725–1730. doi: 10.1056/NEJM199912023412303. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
